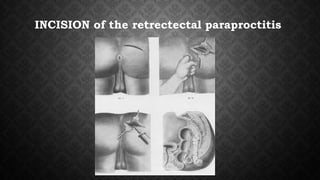
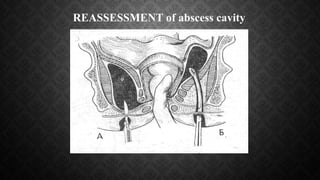
Paraproctitis is an inflammation of the tissue surrounding the rectum that is usually caused by bacteria. It can be acute or chronic. Symptoms depend on the location of the abscess and range from pain and swelling near the anus to fever and abdominal pain. Diagnosis involves a digital rectal exam and sometimes ultrasound or fistulography. Treatment of acute paraproctitis involves surgically opening and draining the abscess, removing infected tissues. Chronic paraproctitis may require additional surgery to remove fistulas. Complications can occur if the infection spreads to nearby organs. Preventing recurrence involves a healthy lifestyle and regular bowel movements.