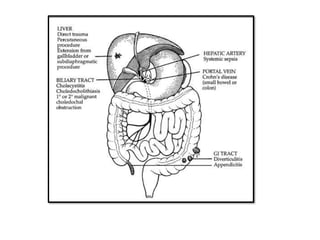
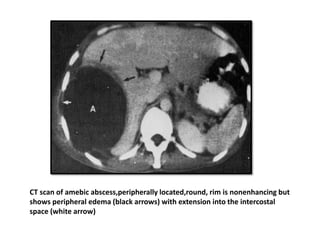
Liver abscesses, primarily pyogenic in nature, arise when the liver's ability to control enteric bacteria is exceeded due to various causes such as trauma or biliary infection. Clinical symptoms include abdominal pain, fever, and jaundice, while diagnosis is aided by imaging techniques like CT scans. Treatment involves abscess drainage, antibiotic therapy, and managing underlying causes to prevent recurrence.