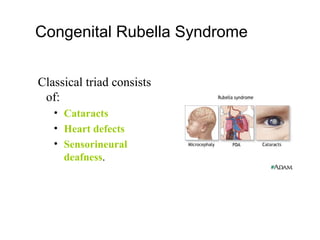
Rubella, also known as German measles, is a viral illness that was first recognized as a distinct disease in 1881. It is caused by the rubella virus, which is transmitted via respiratory droplets. While rubella infection poses little risk to adults, contracting the virus during pregnancy can lead to congenital rubella syndrome in the fetus, causing health issues such as deafness, heart defects, and cataracts. Since the 1960s, effective vaccines have been developed to prevent rubella infection and the risk it poses during pregnancy through universal childhood vaccination programs and antenatal screening of pregnant women.
























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









