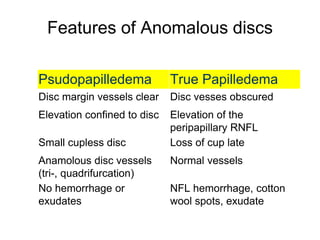
The document discusses the assessment and features of optic discs, particularly focusing on conditions like papilledema and various optical disc anomalies. It highlights the cardinal symptoms of high intracranial pressure and details the diagnostic differences between true papilledema and pseudopapilledema using various imaging techniques. Additionally, it covers the implications of specific anomalies like optic nerve drusen and conditions such as morning glory disc anomaly and optic nerve coloboma.






































































































![fundoscopy and papilledema ophthalmology [2].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/fundoscopyandpapilledema2-250809170746-59ac9d61-thumbnail.jpg?width=640&height=640&fit=bounds)









































