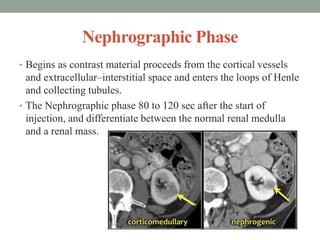
CT urography provides a comprehensive non-invasive evaluation of the urinary tract. It is performed as a multiphase exam, including an unenhanced phase followed by corticomedullary, nephrographic and excretory phases after intravenous contrast administration. The nephrographic phase provides the highest sensitivity for detecting renal masses and abnormalities. Various dose reduction techniques can be used, including lower dose protocols, split-bolus contrast injection, dual-energy CT, and iterative reconstruction. These allow radiation doses to be reduced by up to 80% compared to traditional triple-phase CT urography exams.