







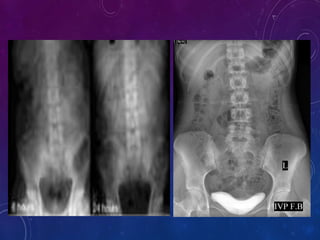


This document discusses intravenous urogram (IVU), a radiographic examination of the urinary tract following contrast media injection, highlighting its historical introduction and decline in usage due to alternatives like CT and ultrasound. It details indications for IVU, possible contraindications, equipment needed, and procedural techniques, including filming techniques and special modifications for various conditions. Advantages and disadvantages of the procedure are also outlined, emphasizing its diagnostic utility while noting risks associated with contrast media.



































































