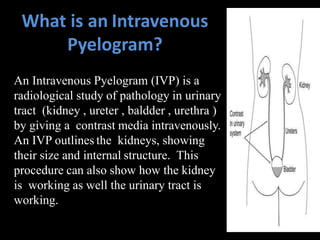
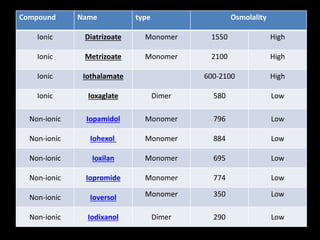
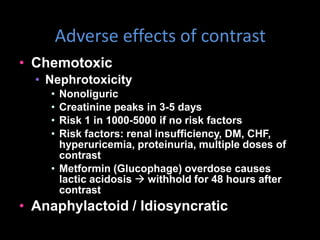
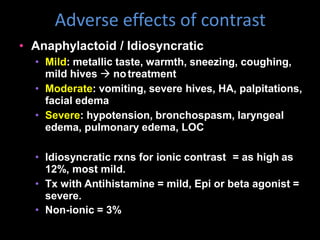
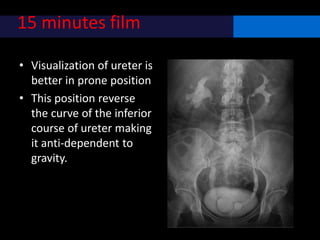
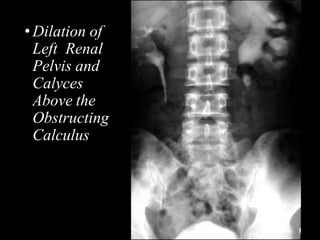
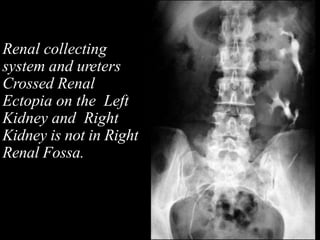
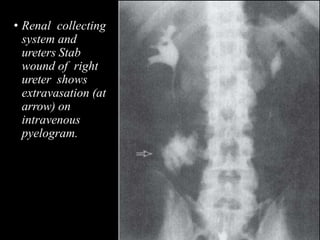
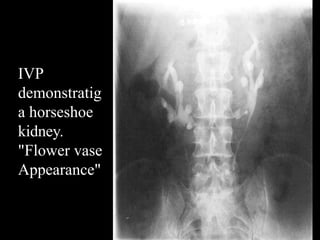
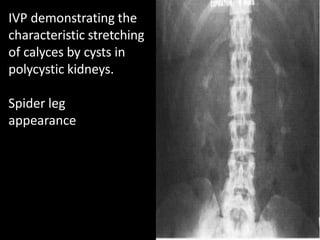
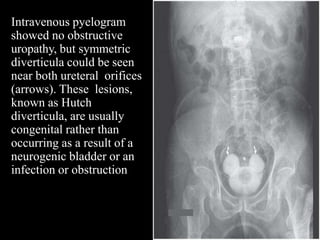
An intravenous pyelogram (IVP) is a radiographic examination of the urinary tract that involves injecting iodinated contrast medium intravenously. An IVP outlines the kidneys and urinary tract, showing their size, structure, and function. It is useful for evaluating conditions like kidney stones, tumors, infections, and anatomical abnormalities. The procedure involves preliminary imaging, injection of contrast, and multiple films over time to visualize different parts of the urinary system as the contrast flows through the kidneys and bladder. Potential risks include adverse reactions to the contrast medium and radiation exposure.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




