Downloaded 148 times

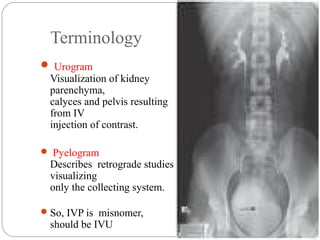
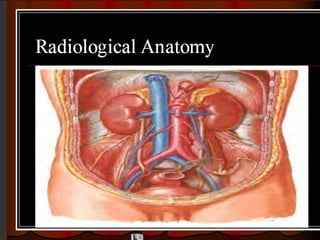

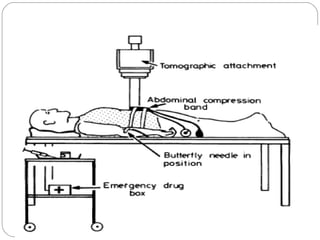
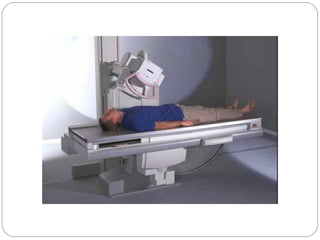

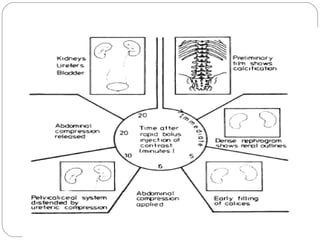

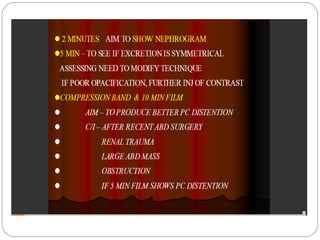

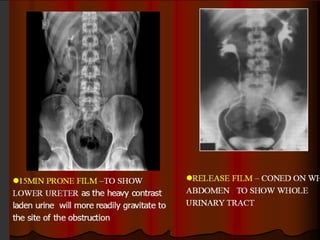
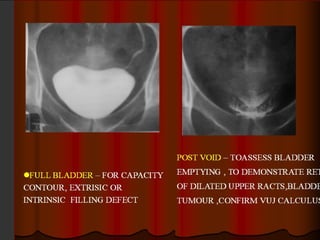

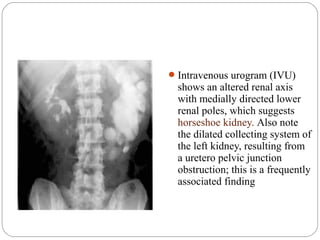








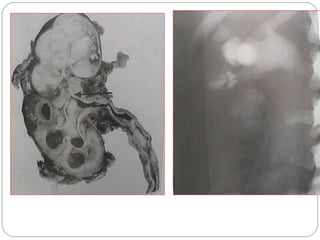




The document discusses intravenous urography (IVU), including its definition, history, indications, contraindications, technique, and what to look for in the images. Some key points: - IVU involves injecting contrast media intravenously and imaging the urinary tract, allowing visualization of the kidneys, ureters, and bladder. - It was introduced in 1929 but use has declined with the rise of CT, ultrasound and MRI. However, it remains useful for visualizing the pelvicalyceal system. - The procedure involves obtaining baseline images, injecting contrast, then timed imaging as the contrast passes through the urinary system, sometimes using compression. Findings are assessed for














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


