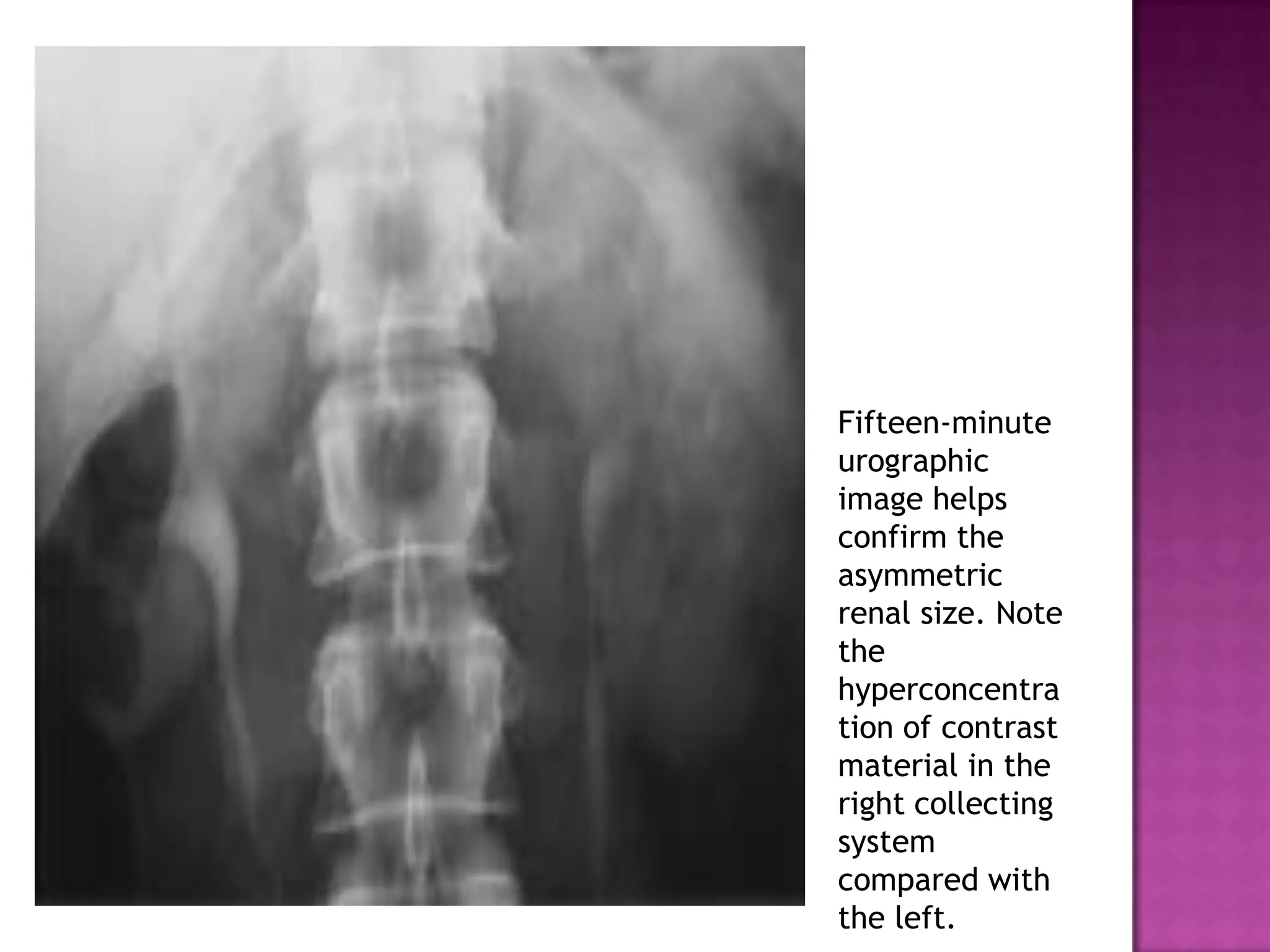
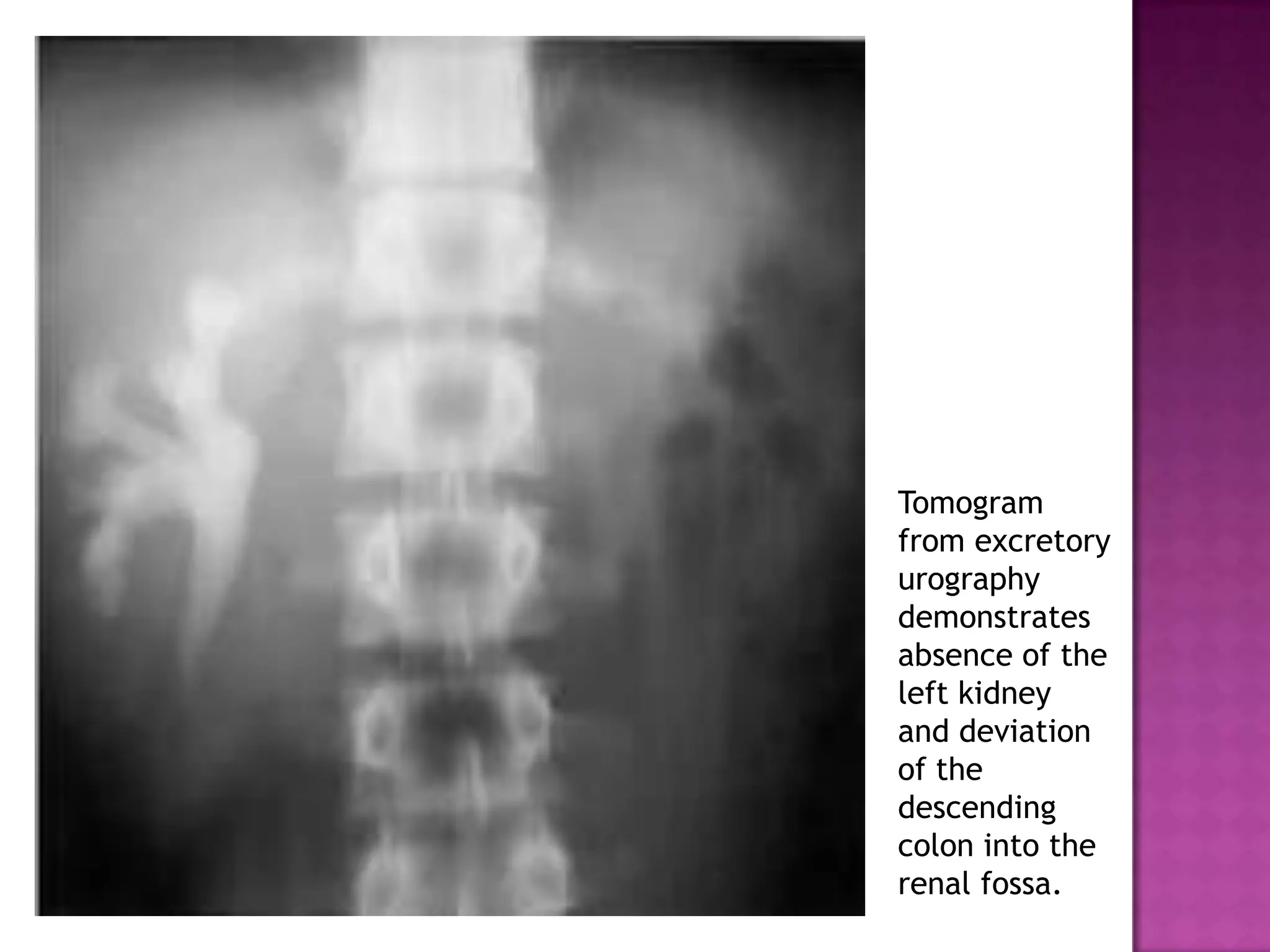
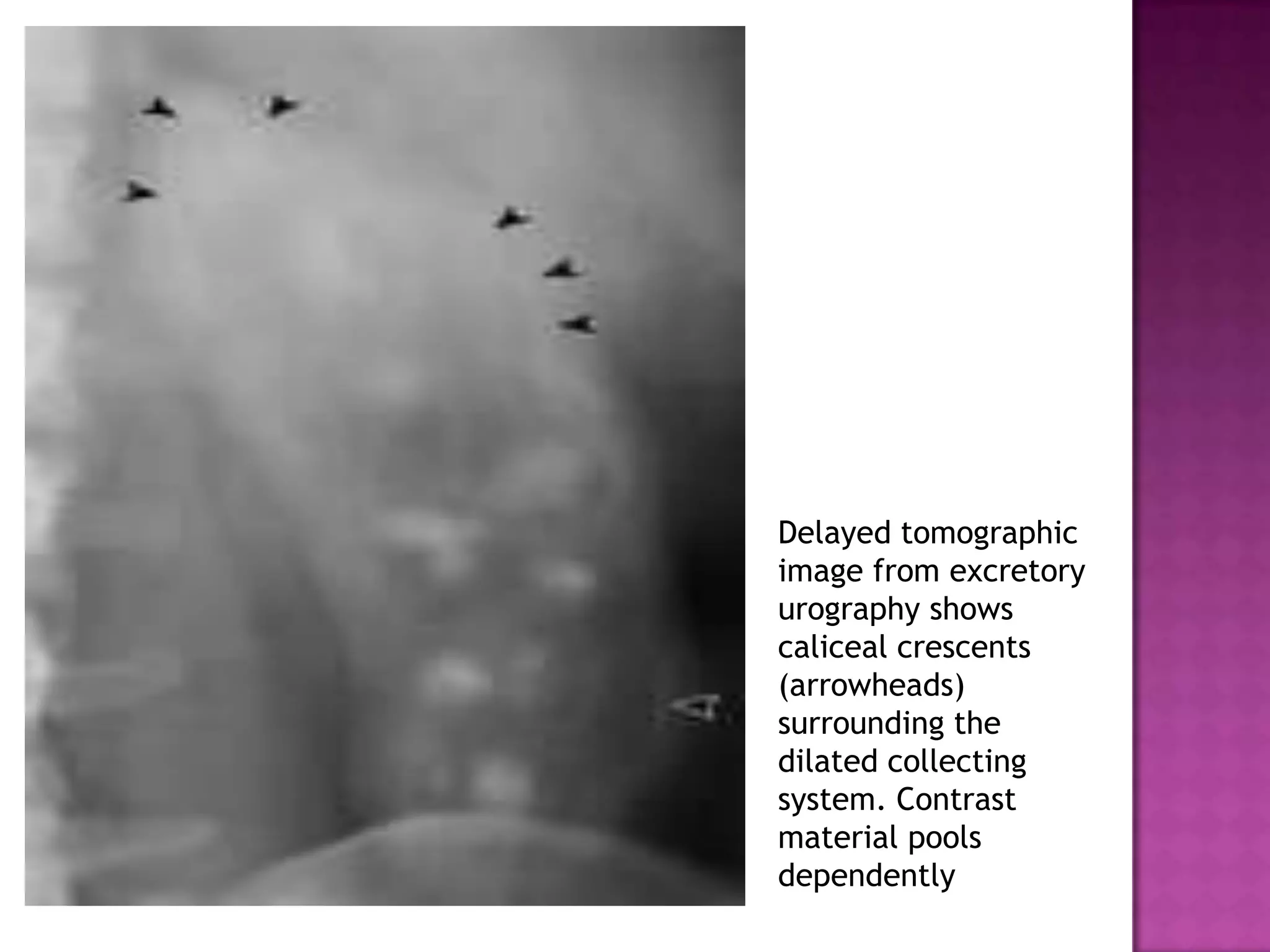
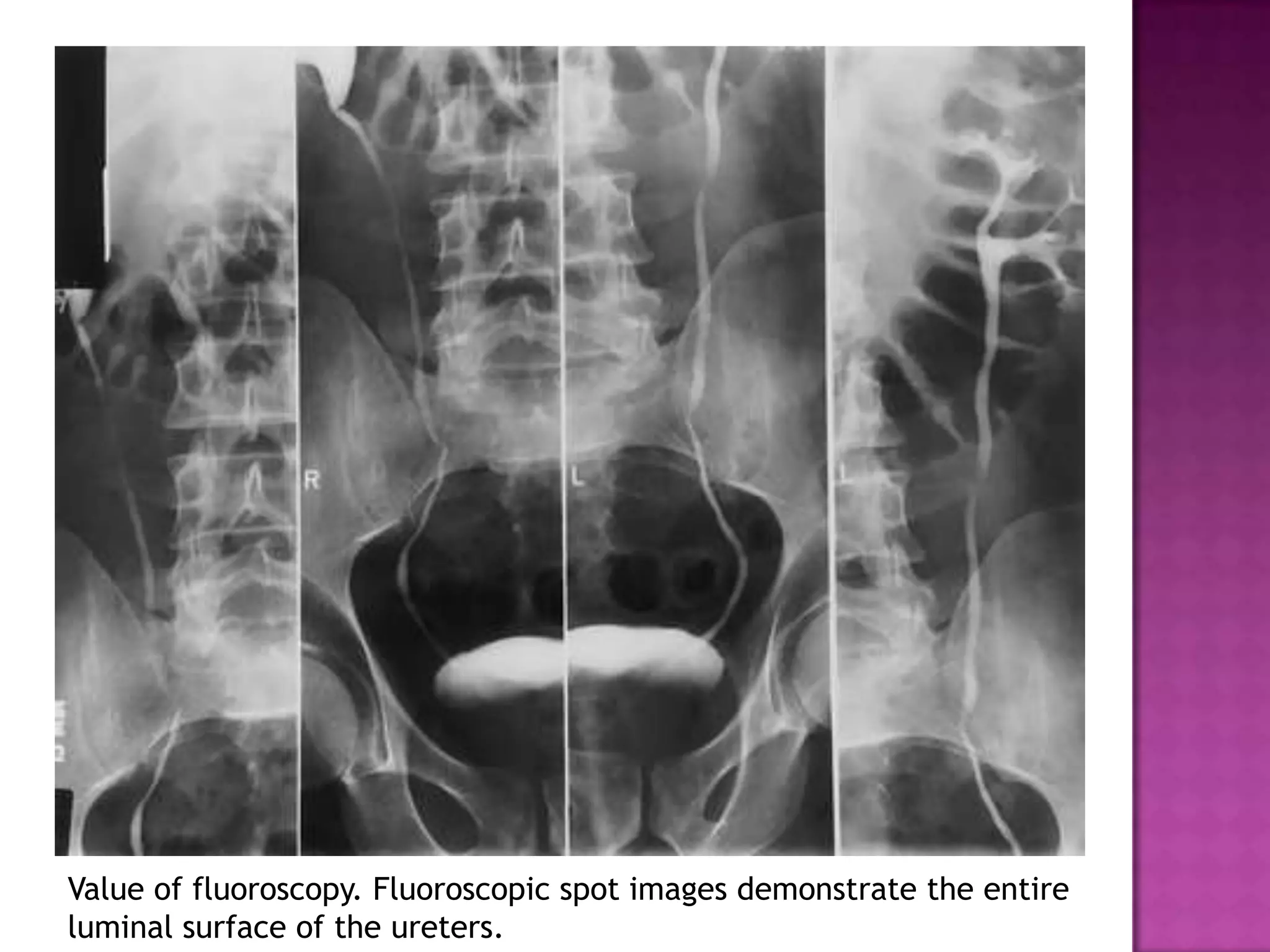
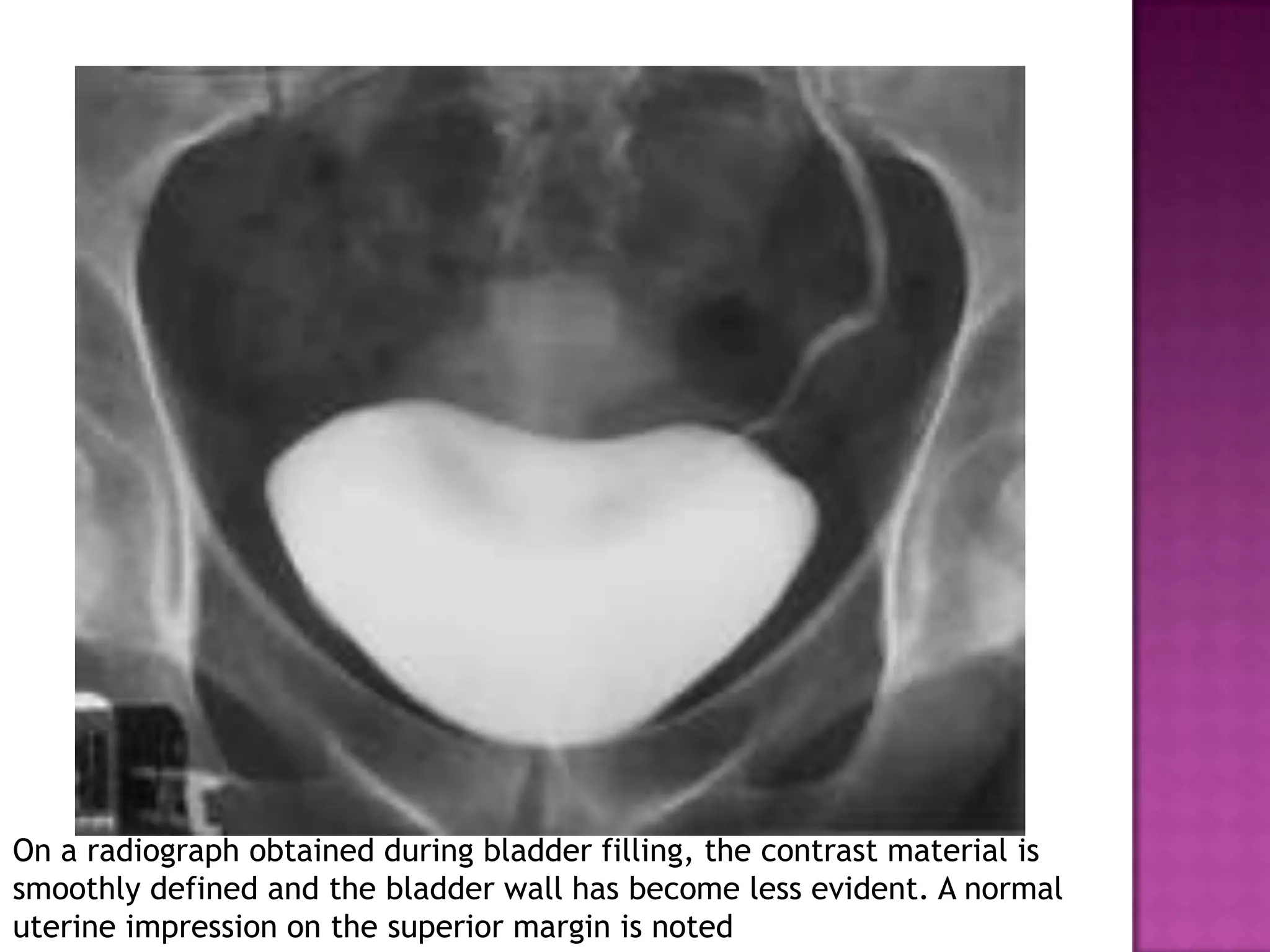
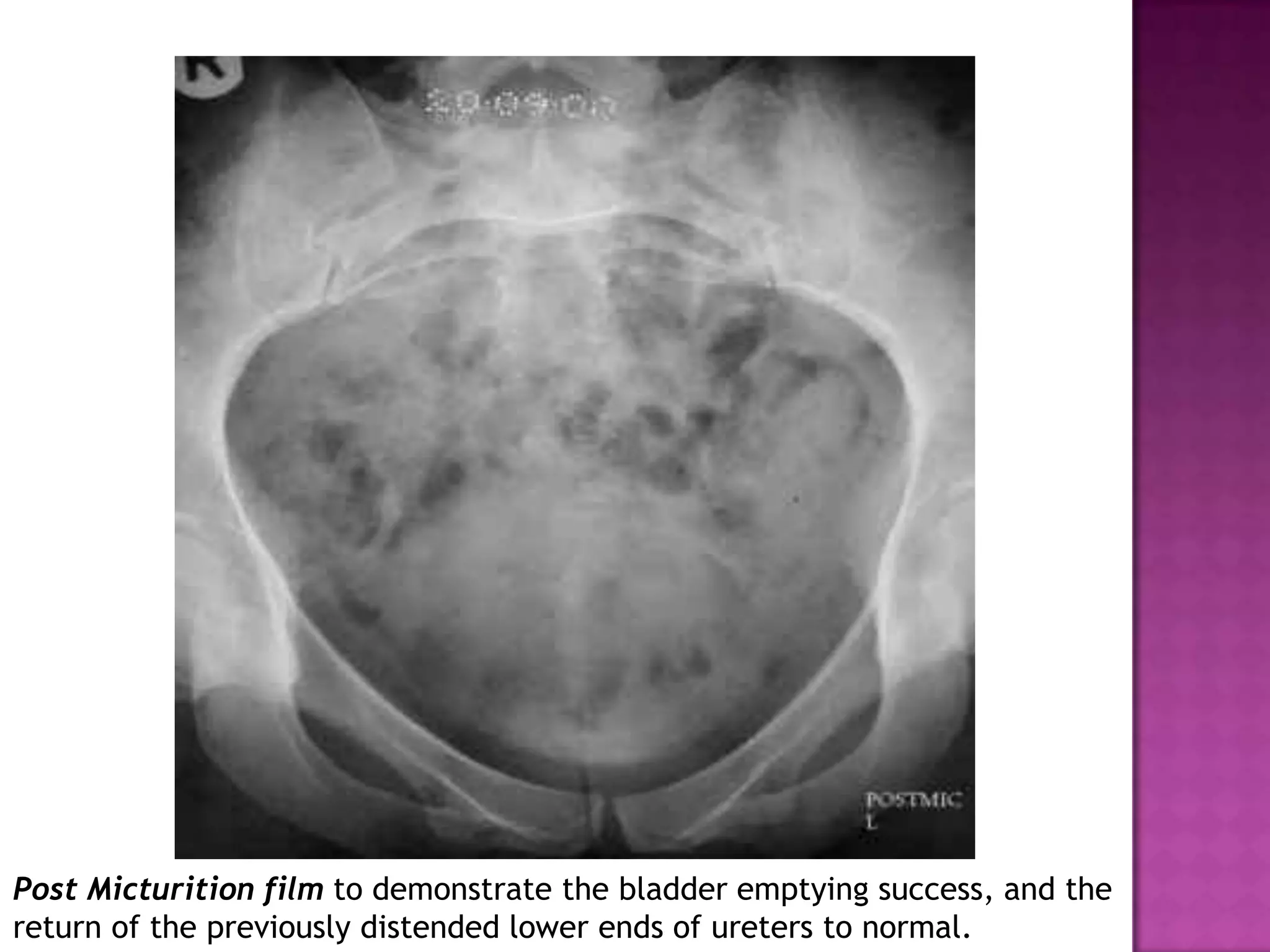
The document discusses excretory urography, which involves administering intravenous contrast and taking timed radiographic images of the urinary system. It describes the indications for excretory urography such as suspected urinary tract pathology or repeated infections. It outlines the procedure, potential findings on images including abnormalities of the kidneys, ureters and bladder, and complications to watch for like contrast reactions. Key phases of kidney imaging and abnormalities that can be identified are also summarized.





![U=([P]xGFR)/Uvol
a-extravasation of contrast
b-absent blood flow :
i-shock
ii-no glomerular filteration :
acute obstruction,infarction](https://image.slidesharecdn.com/excretoryurography-140403112252-phpapp01/75/Excretory-urography-40-2048.jpg)