
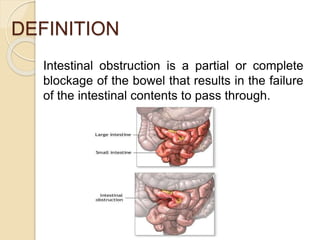

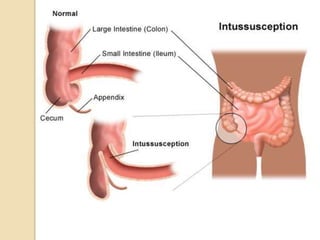
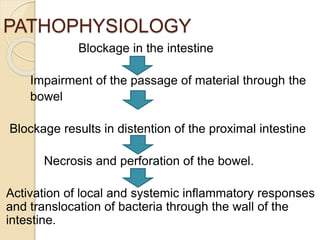
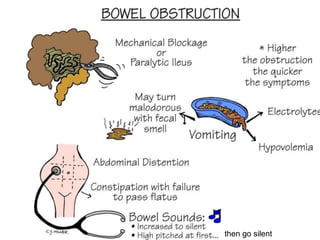
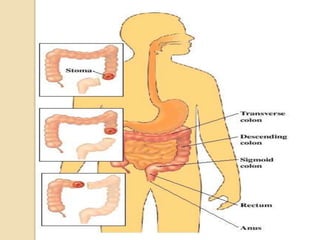


Intestinal obstruction is a serious condition involving a partial or complete blockage of the intestines, which can occur in both small and large intestines, requiring immediate treatment. The document details the types of obstructions (mechanical and functional), their causes, clinical manifestations, diagnostic evaluations, and both medical and surgical management, along with potential complications and nursing assessments. It also includes health education tips for patients experiencing symptoms related to intestinal blockage.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


