DEFINITION
⚫ Partial or
complete
blockageof
the lumen of
the small or
large intestine
causing an
interruption in
the normal
flow of
intestinal
content along
the intestinal
tract.
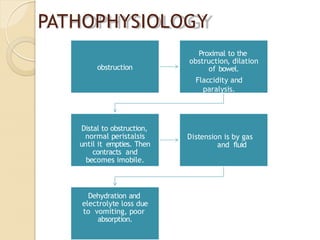
PATHOPHYSIOLOGY
obstruction
Proximal to the
obstruction,dilation
of bowel.
Flaccidity and
paralysis.
Distal to obstruction,
normal peristalsis
until it empties. Then
contracts and
becomes imobile.
Distension is by gas
and fluid
Dehydration and
electrolyte loss due
to vomiting, poor
absorption.
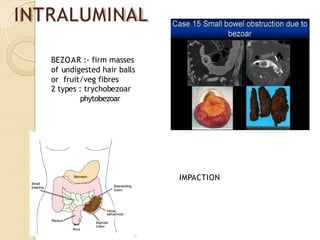
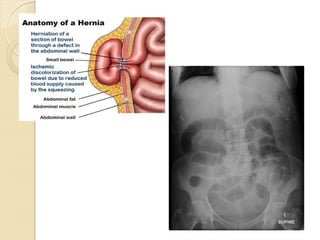
1.
herniation
⚫ Occurs whenpart of small intestine becomes
entrapped in one of theretroperitoneal fossa or in a
congenital mesenteric defect.
⚫ Accounts for 20% of small bowel obstruction.
⚫ Sites :- foramen of winslow, hole in mesentry,
transverse mesocolon or broad ligament.
⚫ Treament :- release the constriction agent by
division
⚫ Peritoneal irritation----- local fibrin
production------ produces adhesions between
apposed surfaces
⚫ As early as 4 weeks post laparotomy.The
majority of patients present between 1-5 years
Colorectal Surgery 25%
Gynaecological 20%
Appendectomy 14%
⚫ Prevention: good surgical technique, washing of the
peritoneal cavity with saline to remove clots, etc,
minimizing contact w/ gauze, covering
anastomosis & raw peritoneal surfaces
12.
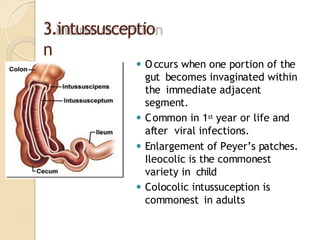
3.intussusceptio
n
⚫ Occurs whenone portion of the
gut becomes invaginated within
the immediate adjacent
segment.
⚫ Common in 1st year or life and
after viral infections.
⚫ Enlargement of Peyer’s patches.
Ileocolic is the commonest
variety in child
⚫ Colocolic intussuception is
commonest in adults
13.
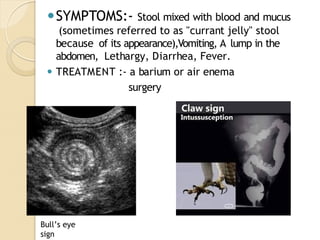
⚫SYMPTOMS:- Stool mixedwith blood and mucus
(sometimes referred to as "currant jelly" stool
because of its appearance),Vomiting, A lump in the
abdomen, Lethargy, Diarrhea, Fever.
⚫ TREATMENT :- a barium or air enema
surgery
Bull’s eye
sign
14.
4.Volvulus
⚫ A twistingor axial rotation of a portion of bowel
about its mesentry. when complete it forms closed
loop obstruction
⚫ ischemia can be primary or secondary:
⚫ 1°: congenital malformation of the
gut(E.G:VOLVULUS NEONATORUM, CECAL OR
SIGMOID VOLVULUS)
⚫ 2°: more common dure to rotation of piece of
bowel around an acquired adhesion or trauma
⚫ Commonest spontaneous type in adults is sigmoid,
can be relieved by decompresion by per anum.
15.
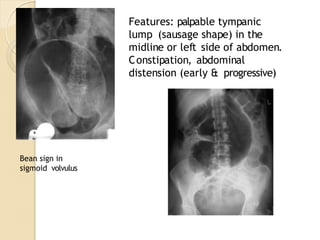
Features: palpable tympanic
lump(sausage shape) in the
midline or left side of abdomen.
Constipation, abdominal
distension (early & progressive)
Bean sign in
sigmoid volvulus
16.
PHYSICAL EXAMINATION
⚫ INSPECTION
Abdominaldistension, scars, visible
peristalsis
⚫ PALPATION
Mass, tenderness, guarding
⚫PERCUSSION
Tympanic ,
dull
⚫ AUSCULTATI
ON
Bowels sounds
are high
pitched.
17.
CLINICAL FEATURES
• Crampy,intermittent, progressive abdominal pain and inability to have a bowel
movement or to pass flatus are common presenting complaints.
• Vom-iting, bilious in proximal obstructions and feculent in distal obstruction, is
usually present.
• Patients with partial SBO can still pass flatus. Physical signs vary from abdominal
distention, localized or general tenderness, to obvious signs of peritonitis.
• Localization of pain and the presence of abdominal surgical scars, hernia, or
masses may provide clues to the site of obstruction.
• The abdomen may be tympanitic to percussion. Active, high-pitched bowel
sounds can be heard in mechanical SBO.
• Bowel sounds may be diminished or absent if the obstruction has been present
for many hours. Rectal examination may demonstrate fecal impaction, rectal
carcinoma, or occult blood.
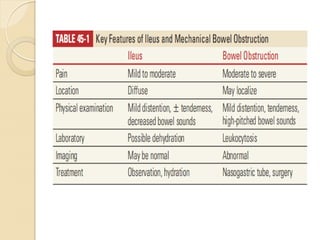
• Key features of ileus and mechanical bowel obstruction are described :
• The presence of stool in the rectum does not exclude obstruction. Consider a
pelvic examination in women. Systemic symptoms and signs depend on the
extent of dehydration and the presence of bowel necrosis or infection.
19.
WORKUP
• Laboratory testsmay include a complete blood count, electrolytes,
blood urea nitrogen, creatinine, lactate levels, coagulation profile, and
type and cross-match. Suspect abscess, gangrene, or peritonitis if
leukocytosis >20,000 or left shift is noted.
• An elevated hematocrit is consistent with dehydration.
• Flat and upright abdominal radiographs and an upright chest x-ray can
screen for obstruction (see Fig. 45-1), confirm severe constipation, or
diag_x0002_nose hollow viscous perforation with free air.
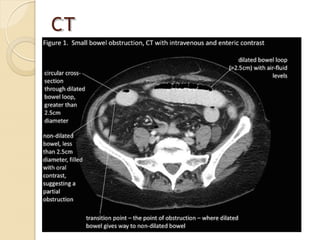
• The diagnostic procedure of choice in the ED is CT scanning using IV
and oral contrast when possible.
• CT scanning can delineate partial versus complete bowel obstruction,
partial SBO versus ileus, and strangulated versus simple SBO.
20.
RADIOLOGICAL EXAMINATION
⚫ Plainabdominal X ray
⚫ USS ( free fluid, masses, mucosal folds,
patterns of peristalsis, doppler of mesenteric
vasculature, solid organs)
⚫ other advanced studies(CT, MRI, contrast
studies)
ED care isdirected at vigorous fluid resuscitation with crystalloids, careful
monitoring of response, and prompt surgical consultation. Surgical
inter_x0002_vention is usually necessary to treat a mechanical obstruction.
1. Decompress the bowel with a nasogastric tube especially if vomiting or
distension is present.
2. Administer preoperative broad-spectrum intravenous antibiotics
cov_x0002_erage such as piperacillin/tazobactam 3.375 g IV every 6 hours,
tircarcillin-clavulanate 3.1 g IV every 6 hours or ampicillin/sulbac_x0002_tam
3.0 g or double drug coverage with cefotaxime 2 g or ceftriax_x0002_one 2 g
plus clindamycin 600 mg or metronidazole 1 g or a
carbapenem, such as meropenem 1 g IV every 8 hours.
3. When the diagnosis is uncertain or if adynamic ileus is suspected,
con_x0002_servative measures, such as intravenous fluids and observation
without
surgical intervention, may be appropriate.
4. In patients with pseudoobstruction, colonoscopy is both diagnostic and
therapeutic. Surgery is not indicated.
EMERGENCY CARE:
25.
COMPLICATIONS
⚫ Include excessivebleeding
⚫ infection
⚫ Formation of abscesses
⚫ leakage of stool from
anastomosis
⚫ adhesion formation
⚫ paralytic ileus
⚫ Reoccurrence of the
obstruction
PARALYTIC ILEUS
⚫ Obstructionof the intestine due to paralysis of the
intestinal muscles.The paralysis does not need to
be complete to cause ileus, but the intestinal muscles
must be so inactive that it prevents the passage of
food and leads to a functional blockage of the
intestine.
⚫ Most often occurs after surgery but can also occur
due to an inflammatory response, electrolyte
abnormality, thoracic or lumbar spinal fractures
28.
TYPE
S
⚫ Postoperative :-a degree of ileus usually occurs after
any abdominal procedure and is usually self limiting,
with a variable duration of 24-72 hours.
⚫ Infection :- intra abdominal sepsis may give rise
to localised or generalized ileus.
⚫ Reflex ileus :-this may occur following fractures of
spine or ribs and retroperitoneal hemmorrhage.
⚫ Metabolic:- uremia or hypokalemia are most
common contributing factor.
29.
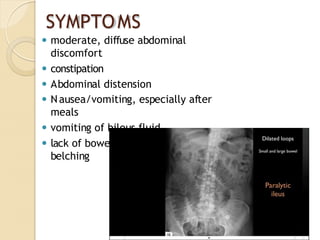
SYMPTOMS
⚫ moderate, diffuseabdominal
discomfort
⚫ constipation
⚫ Abdominal distension
⚫ Nausea/vomiting, especially after
meals
⚫ vomiting of bilous fluid
⚫ lack of bowel movement excessive
belching
30.
MANAGEMENT
⚫ Essence ofmanagement---- prevention with use of
nasogastric and restriction of oral intake until
bowel sounds and passage of flatus returns
maintain electrolyte balance
⚫ SPECIFIC TREATMENT:
1. remove primary cause
2. decompressed GI distension
⚫ if prolonged paralytic ileus,
1. consider laprotomy
2. exclude hidden cause and
facilitate bowel decompression