Downloaded 115 times





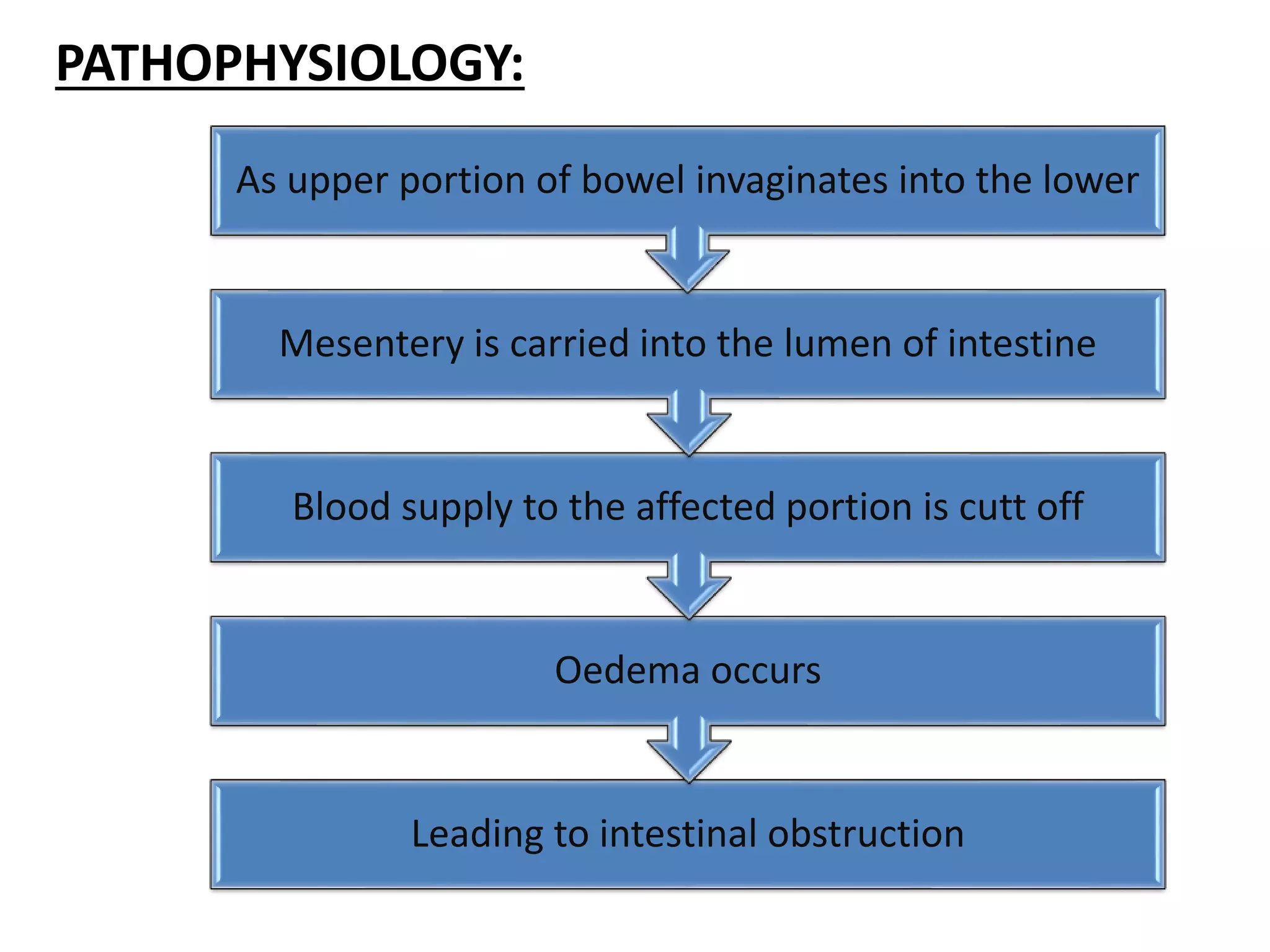





This document discusses intestinal obstruction and intussusception. Intestinal obstruction is defined as a mechanical or functional blockage of the intestines. Common causes of small bowel obstruction include adhesions, Crohn's disease, and volvulus. Large bowel obstruction may be caused by inflammatory bowel disease, constipation, or colon atresia. Intussusception is the telescoping of one segment of intestine into another, and accounts for 1-4 cases per 1000 live births. Clinical features of intestinal obstruction and intussusception include abdominal pain, vomiting, distention, and constipation. Diagnostic tests include blood tests, imaging like CT scans and ultrasound. Surgical management is often needed to correct the obstruction























































































