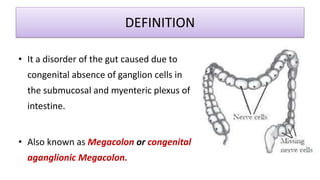
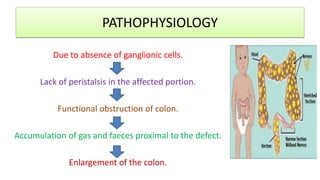


Hirschsprung's disease is a disorder of the gut caused by the congenital absence of ganglion cells in the intestine. It occurs in around 1 in 500 live births and is more common in males. Symptoms in neonates include failure to pass meconium and abdominal distension. In older children, symptoms include constipation and foul-smelling stools. Diagnosis involves tests like barium enema and rectal biopsy. Treatment consists of medical management with enemas or surgery to remove the affected segment and reconnect the intestine. Nursing care focuses on monitoring for complications pre-and post-surgery and providing bowel care.




















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

