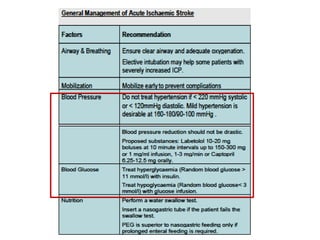
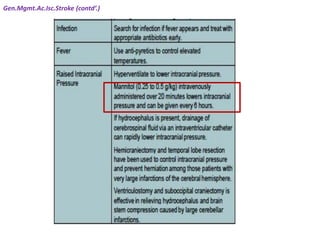
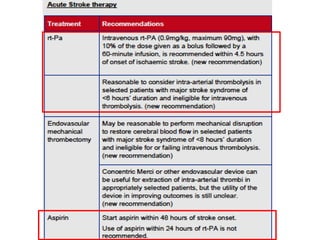
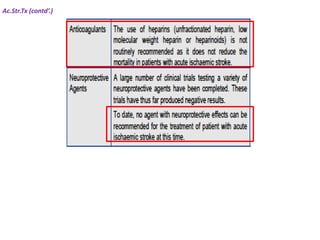
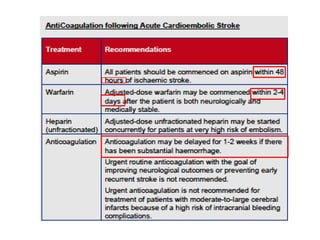
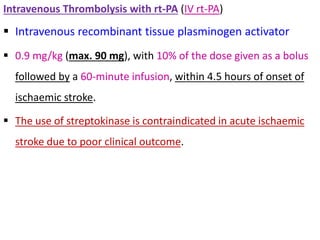
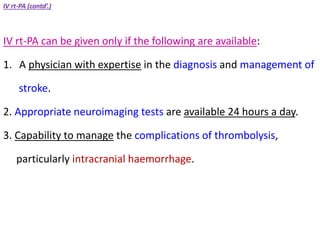
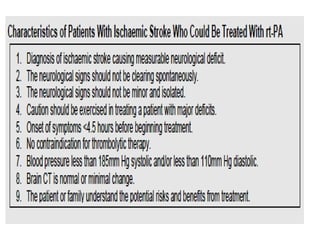
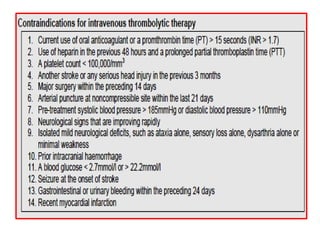
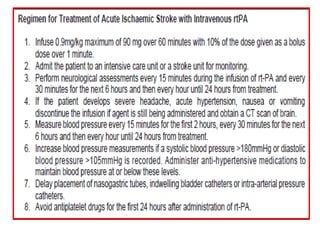
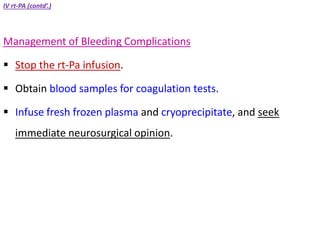
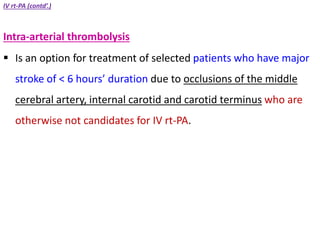
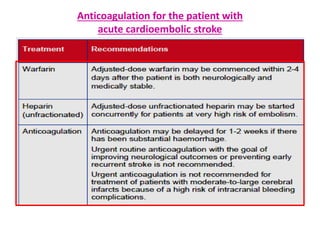
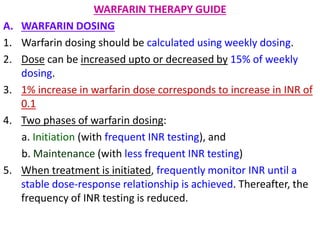
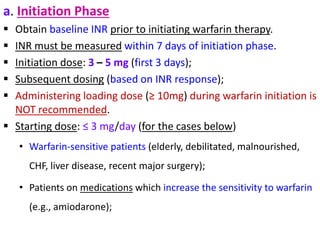
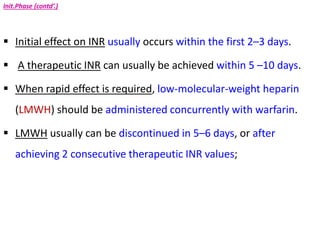
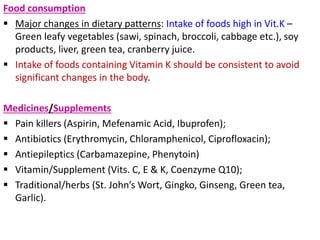
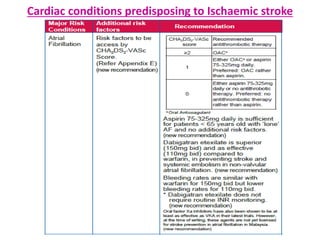
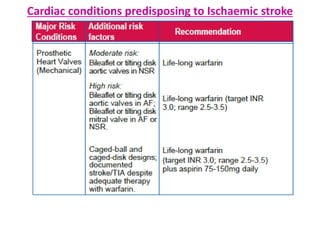
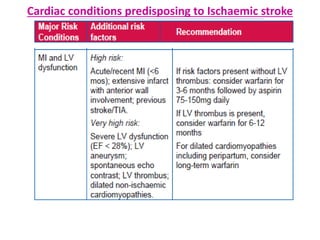
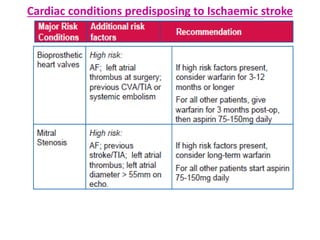
The document provides guidelines for the pharmacotherapy of ischemic stroke. It discusses the causes, signs and symptoms, and risk factors for ischemic stroke. It also outlines the management of acute ischemic stroke, including indications for intravenous thrombolysis with rt-PA and intra-arterial thrombolysis. The CHA2DS2-VASc and HAS-BLED scores for assessing stroke and bleeding risk in atrial fibrillation are also covered. The document provides detailed guidance on anticoagulation therapy for stroke prevention, including warfarin dosing, monitoring, and management.
![PHARMACOTHERAPY POINTERS FOR
ISCHEMIC STROKE
[MALAYSIAN CPGs]](https://image.slidesharecdn.com/pharmacotherapypointersforischemicstrokemalaysiancpgs-230519035129-300dc0e5/85/PHARMACOTHERAPY-POINTERS-FOR-ISCHEMIC-STROKE-MALAYSIAN-CPGs-pdf-1-320.jpg)

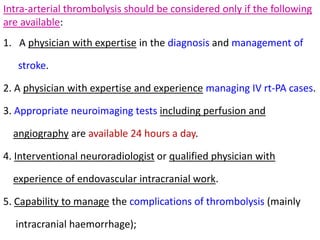
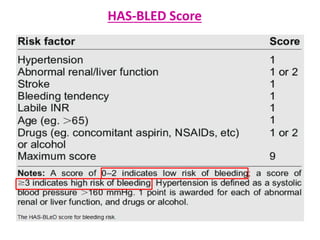
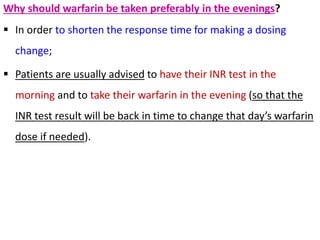
![HAS-BLED Score
HTN, Abnormal renal/liver function, Stroke, Bleeding history or
predisposition, Labile INR, Elderly (age > 65), and Drugs/alcohol
concomitantly;
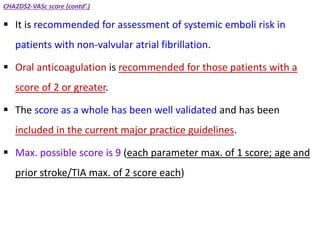
To estimate the 1-year risk for major bleeding in patients with
atrial fibrillation;
Max. possible score is 9 [1 point for each of the components
(abnormal renal/liver function and drugs/alcohol possibly scoring
2 points each if both are present)].
‘Drugs’ refer to any medications that increase bleeding risk during
anticoagulation (aspirin, NSAIDs, steroids);
‘Alcohol’ refers to alcohol abuse.](https://image.slidesharecdn.com/pharmacotherapypointersforischemicstrokemalaysiancpgs-230519035129-300dc0e5/85/PHARMACOTHERAPY-POINTERS-FOR-ISCHEMIC-STROKE-MALAYSIAN-CPGs-pdf-27-320.jpg)
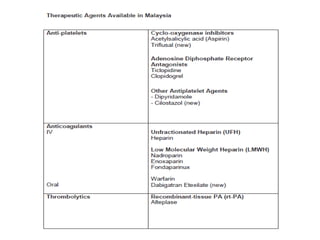
![Few General Pointers
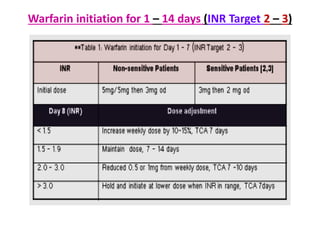
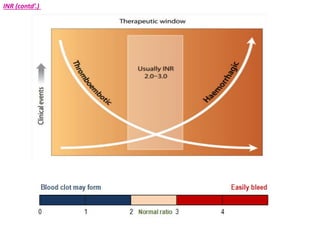
Recommended warfarin dose INR target 2.5 [range 2.0 to 3.0]
unless stated otherwise
Increase BP measurements if a systolic BP >180mmHg or
diastolic BP >105mmHg is recorded. Administer anti-
hypertensive medications to maintain BP at or below these
levels.
ICSI guideline - Increase of 15% weekly dose of warfarin
would correspond to increase in INR of 1.0.](https://image.slidesharecdn.com/pharmacotherapypointersforischemicstrokemalaysiancpgs-230519035129-300dc0e5/85/PHARMACOTHERAPY-POINTERS-FOR-ISCHEMIC-STROKE-MALAYSIAN-CPGs-pdf-55-320.jpg)

































![PHARMACOTHERAPY POINTERS FOR ANXIETY & AFFECTIVE DISORDERS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforanxietyaffectivedisordersmalaysiancpgs-230519033737-7916c3bc-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR SCHIZOPHRENIA [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforschizophreniamalaysiancpgs-230519020539-71314b89-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR ATHEROSCLEROSIS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforatherosclerosismalaysiancpgs-230519014441-00a85dfd-thumbnail.jpg?width=640&height=640&fit=bounds)

![Interpretation of Clinical Lab Data [PFTs] for Newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatapftsfornewbies-230518072330-48aef17c-thumbnail.jpg?width=640&height=640&fit=bounds)
![Interpretation of Clinical Lab Data [CARDIAC] for newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatacardiacfornewbies-230518071258-e33c3626-thumbnail.jpg?width=640&height=640&fit=bounds)

![TDM POINTERS [GERIATIC & PAEDIATRIC PATIENTS].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/tdmpointersgeriaticpaediatricpatients-230518044517-7b716179-thumbnail.jpg?width=640&height=640&fit=bounds)