This document summarizes the pathophysiology, clinical features, diagnosis, and management of salicylate and paracetamol poisoning.
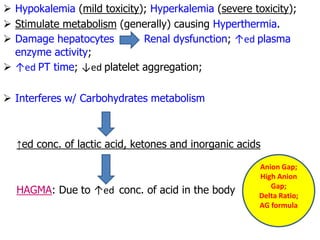
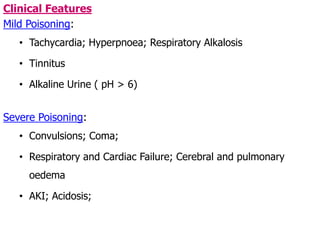
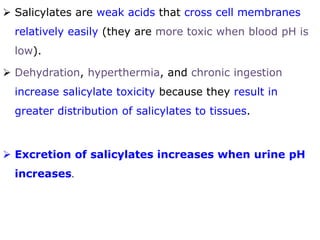
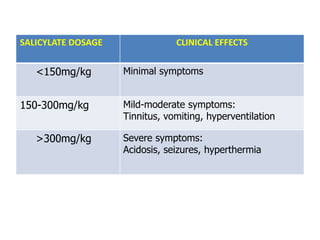
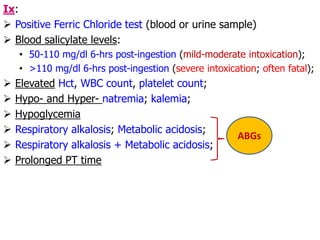
It describes how salicylates cause respiratory alkalosis by stimulating respiration and how this leads to hypokalemia, dehydration, and other effects. Clinical features range from mild tachycardia with high doses to seizures, coma, and organ failure. Diagnosis involves blood or urine tests and treatment includes gastric lavage, activated charcoal, alkalinization, and hemodialysis if needed.
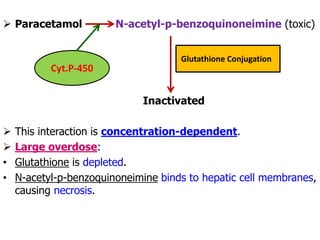
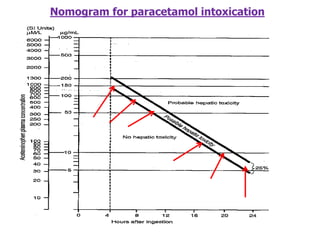
For paracetamol, it explains how toxicity occurs when glutathione is depleted, allowing a toxic metabolite to damage the liver. Symptoms appear within

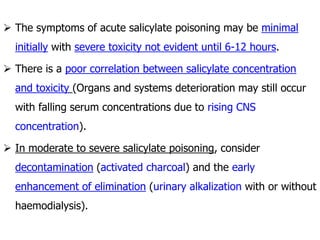
![ Salicylate poisoning is mainly due to ingestion of…
• Aspirin [10-20 g (adults); 3g (children)], or
• LMS (1 ml of 25% LMS = 300 mg salicylate)
Pathophysiology:
SALICYLATES
Stimulate resp.
centre
Hyperpnoea
(hyperventilation)
Hypocarbia
(Hypocapnoea)
↓ed CO2;
↑ed HCO3
-
↑ed pH
Respiratory
Alkalosis
Body compensates:
Excretes HCO3
-, Na+,
Ca2+; BUT…
Retains Cl-
Hypokalemia and
dehydration](https://image.slidesharecdn.com/tdmpointers-salicylatesparacetamolpoisoning-230518070500-c76cb9e4/85/TDM-Pointers-Salicylates-Paracetamol-Poisoning-pdf-2-320.jpg)





















































![PHARMACOTHERAPY POINTERS FOR ISCHEMIC STROKE [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforischemicstrokemalaysiancpgs-230519035129-300dc0e5-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR ANXIETY & AFFECTIVE DISORDERS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforanxietyaffectivedisordersmalaysiancpgs-230519033737-7916c3bc-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR SCHIZOPHRENIA [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforschizophreniamalaysiancpgs-230519020539-71314b89-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR ATHEROSCLEROSIS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforatherosclerosismalaysiancpgs-230519014441-00a85dfd-thumbnail.jpg?width=640&height=640&fit=bounds)

![Interpretation of Clinical Lab Data [PFTs] for Newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatapftsfornewbies-230518072330-48aef17c-thumbnail.jpg?width=640&height=640&fit=bounds)
![Interpretation of Clinical Lab Data [CARDIAC] for newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatacardiacfornewbies-230518071258-e33c3626-thumbnail.jpg?width=640&height=640&fit=bounds)
![TDM POINTERS [GERIATIC & PAEDIATRIC PATIENTS].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/tdmpointersgeriaticpaediatricpatients-230518044517-7b716179-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









