This document provides an overview of hepatic function tests and their interpretation. It discusses the three main categories of liver function tests - tests of excretion, evaluation of synthesis, and enzyme activity evaluation. Key liver enzymes include bilirubin, albumin, prothrombin time, AST, ALT, ALP, GGT, and LDH. Elevations in certain enzymes can indicate hepatocellular injury, cholestasis, or other liver conditions. The ratios of ALT to AST and ALP to GGT are also important for determining the underlying cause of liver dysfunction.
Liver isthe largest organ in the body (1.2-1.5 kgs.).
2 sources of blood supply to the liver:
• Hepatic artery (from the aorta; supplies O2-rich arterial blood);
• Portal veins (venous outflow of intestine and spleen);
Hepatic Function Tests (LFTs)
Most often used to determine:
• Presence and type of liver disease;
• Extent and progression of liver disease;
LFTs analyze:
1] Test of excretion by the liver
Reported as:
• Total Bilirubin [ Unconjugated (Indirect) + Conjugated (Direct)]
• Direct Bilirubin (Conjugated)
3.
2] Evaluation ofsynthesis in
the liver
Albumin
Pre-albumin
Globulin
Total Protein
Prothrombin time
Cholesterol & esters
3] Enzyme activity evaluation
Serum transaminases
* AST (SGOT)
* ALT (SGPT)
Serum alkaline phosphatase
[ALP]
Lactate Dehydrogenase
[LDH]
ɣ-glutamyl transpeptidase
[GGTP]
4.
Serum Bilirubin:
Isa breakdown product of Hb; is predominant in the bile;
• Indirect form (bound to albumin; H2O-insoluble );
• Direct form (secreted into bile);
Hepatobiliary function + RBC turnover rate determines the
extent of bilirubin conjugation and excretion.
Hyperbilirubinaemia may not always cause clinically apparent
jaundice (usually visible >60 umol/l).
Unconjugated bilirubin is water-insoluble (doesn’t affect the
patient’s urine colour);
Conjugated bilirubin can pass into the urine (as urobilinogen,
causing the urine to become darker).
5.
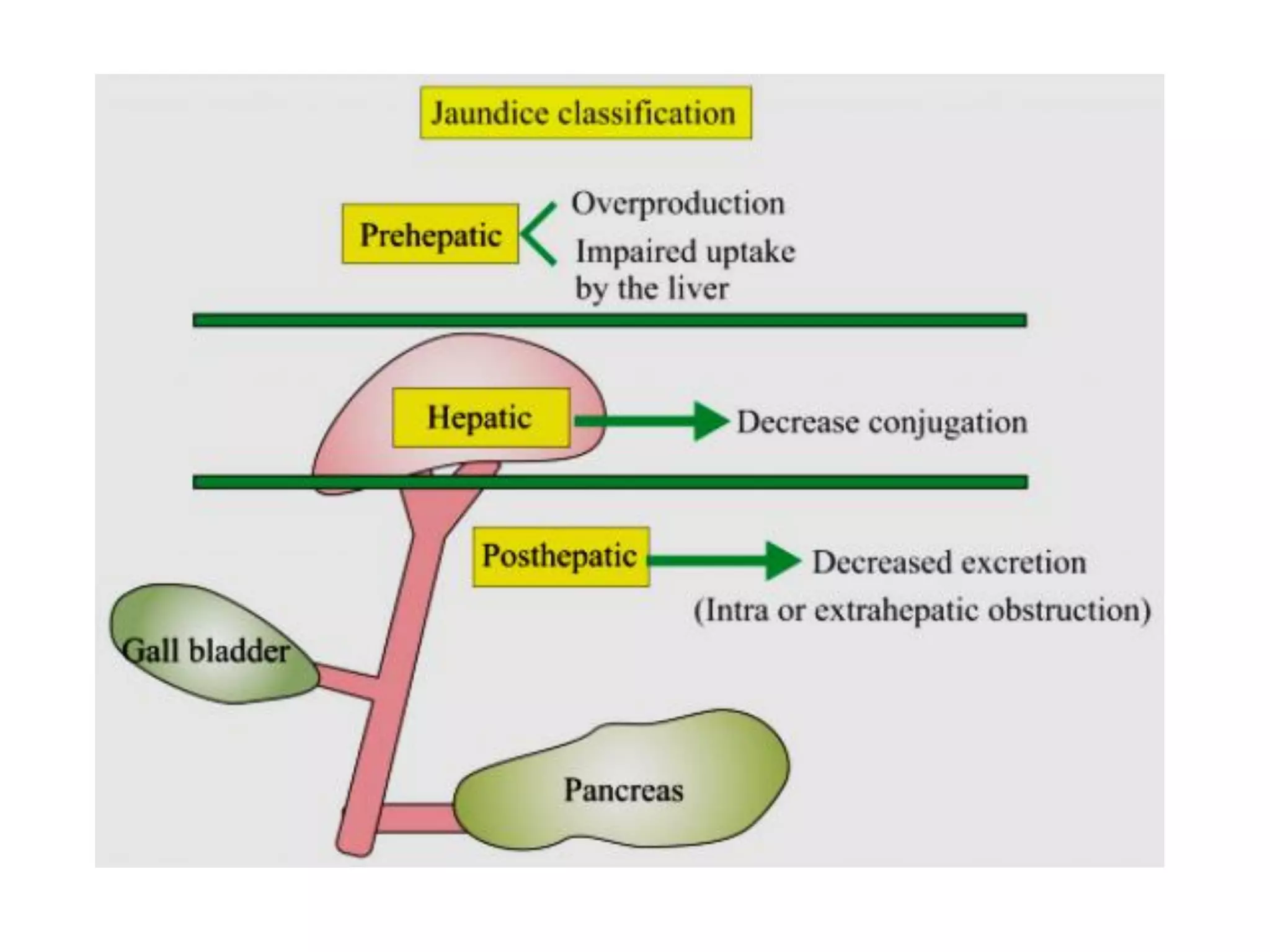
Combination ofthe urine colour and stools indicate the cause
of jaundice:
• Normal urine + normal stools = pre-hepatic cause
• Dark urine + normal stools = hepatic cause
• Dark urine + pale stools = post-hepatic cause (obstructive)
Unconjugated hyperbilirubinaemia (causes):
• Haemolysis (haemolytic anaemia)
• Impaired hepatic uptake (drugs, congestive cardiac failure)
• Impaired conjugation (Gilbert’s syndrome)
Conjugated hyperbilirubinaemia (causes):
• Hepatocellular injury
• Cholestasis
6.
Albumin
Synthesized inthe liver;
Helps to bind water, cations, fatty acids, and bilirubin;
Helps to maintain oncotic pressure of blood.
↓ed Albumin (causes):
• Liver disease (e.g. cirrhosis);
• Inflammation – triggers acute phase response – temporarily
decreases albumin production by liver;
• Protein-losing enteropathies or nephrotic syndrome;
7.
Prothrombin time (PT)
Is a measure of the blood’s coagulation tendency;
↑ed PT (in absence of other 2° causes such as anticoagulant drug use
and vitamin K deficiency) indicates liver disease and dysfunction.
The liver is responsible for the synthesis of clotting factors. So,
hepatic pathology can impair this process resulting in ↑ed PT time.
AST/ALT ratio
Used to determine the likely cause of LFT derangement:
ALT > AST (a/w chronic liver disease);
AST > ALT (a/w cirrhosis and acute alcoholic hepatitis);
• What about ASpartate aminoTransferase?
8.
ALanine Amino Transferase(ALT)
Highly concentrated within hepatocytes;
Enters the blood after hepatocellular injury (useful marker or
indicator of hepatocellular injury).
ALkaline Phosphatase (ALP)
Highly concentrated in liver, bile duct and bone tissues;
Often ↑ed in liver pathology due to ↑ed synthesis in response to
cholestasis (useful indirect marker or indicator of cholestasis);
9.
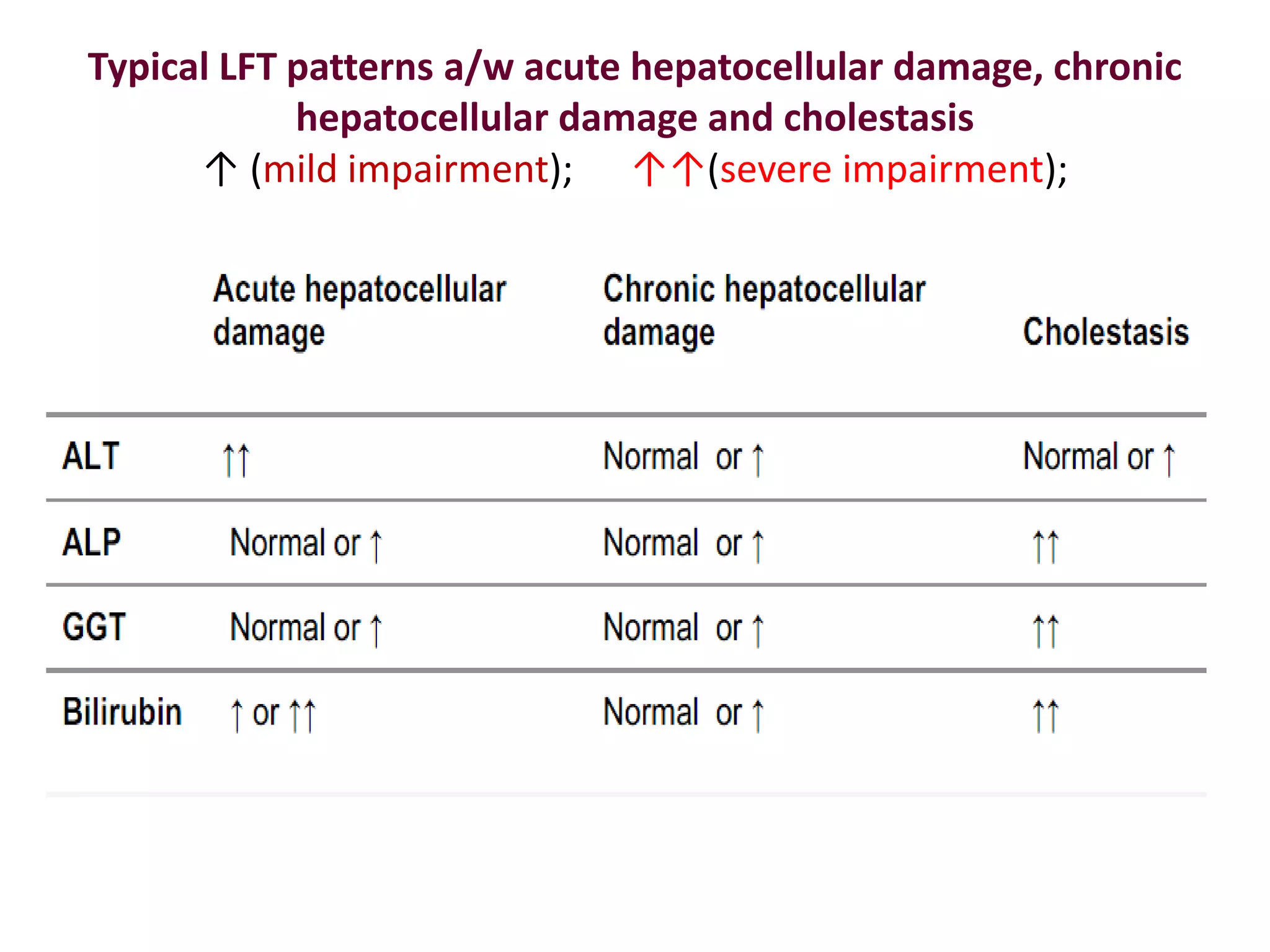
> 10x↑ in ALT and < 3x ↑ in ALP (predominantly hepatocellular
injury);
[E.g., viral hepatitis, metabolic liver diseases, drug or alcohol
toxicity and autoimmune hepatitis]
< 10x ↑ in ALT and > 3x ↑ in ALP (cholestasis);
[E.g., Bile stones, cholestatic drug-induced liver injury]
It is possible for patients to have both hepatocellular injury and
cholestasis.
10.
Gamma-Glutamyl Transferase (GGT)
If ALP ↑es, then it is important to review the level of GGT.
↑ed GGT:
• biliary epithelial damage and bile flow obstruction;
• in response to alcohol and drugs (phenytoin);
A markedly ↑ed ALP + ↑ed GGT is highly suggestive of cholestasis.
11.
Isolated ↑ ALP
↑ ALP + normal GGT (suspicion of non-hepatobiliary pathology);
ALP is also present in bone (anything that leads to ↑ed bone
breakdown can ↑ ALP).
Isolated ↑ ALP (causes):
• Bony metastases or primary bone tumours (e.g. sarcoma)
• Vitamin D deficiency
• Recent bone fractures; Renal osteodystrophy;
12.
Jaundice patient w/normal ALT and ALP levels
An isolated ↑ in bilirubin (suggestive of pre-hepatic cause of
jaundice);
Isolated ↑ in bilirubin (causes):
• Gilbert’s syndrome (most common cause);
• Haemolysis;
13.
Gluconeogenesis
Is ametabolic pathway resulting in the generation of glucose from
certain non-carbohydrate carbon substrates.
The liver plays a significant role in gluconeogenesis.
Assessment of serum blood glucose can provide an indirect
assessment of the liver’s synthetic function.
Gluconeogenesis is one of the last functions to become impaired
in the context of liver failure.
Acute hepatocellular injury(common causes):
Poisoning (paracetamol overdose)
Infection (Hepatitis A and B)
Liver ischaemia
Chronic hepatocellular injury (common causes):
Alcoholic fatty liver disease
Non-alcoholic fatty liver disease
Chronic infection (Hepatitis B or C)
Primary biliary cirrhosis
16.
IMPORTANT POINTERS
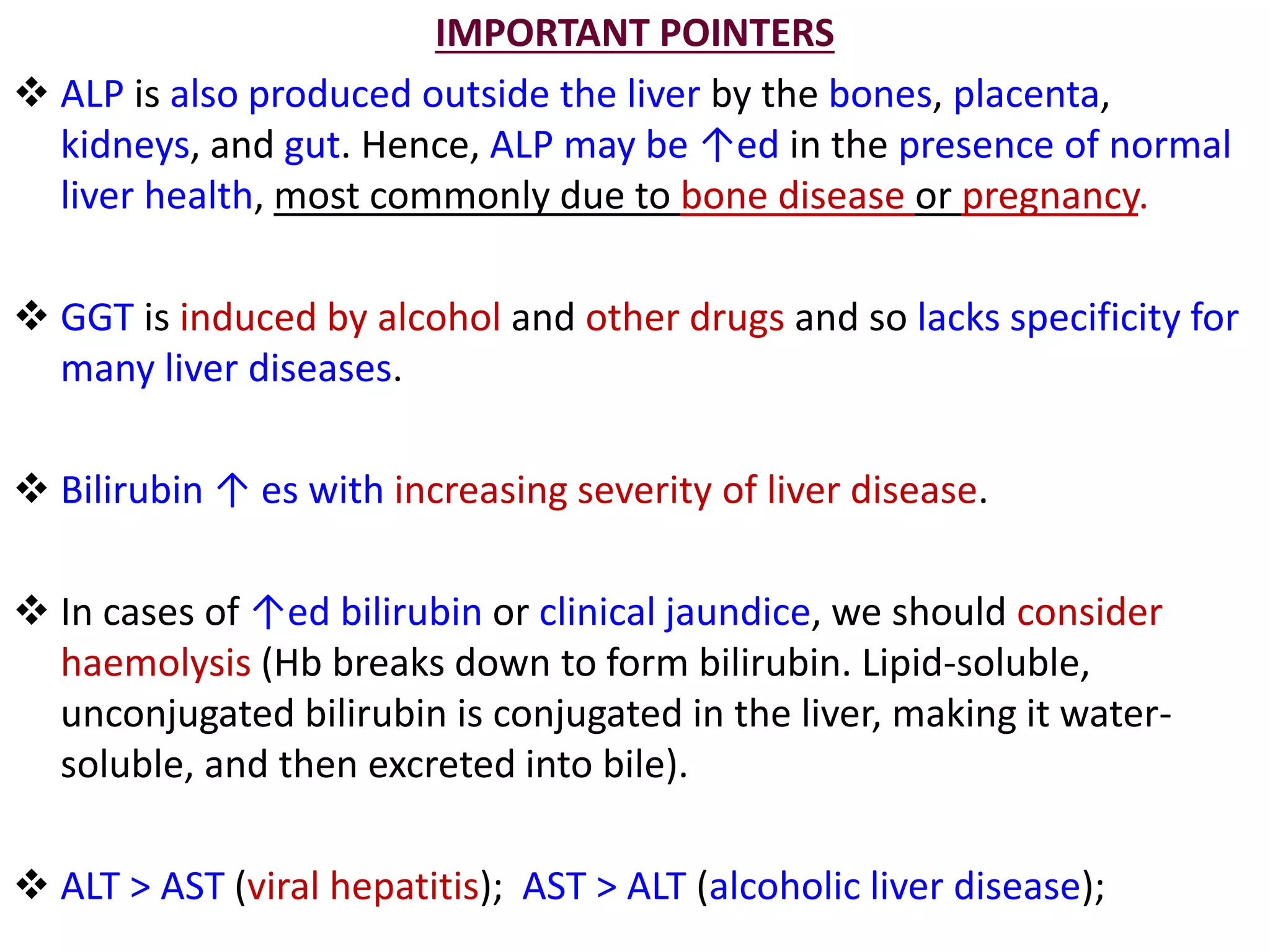
ALPis also produced outside the liver by the bones, placenta,
kidneys, and gut. Hence, ALP may be ↑ed in the presence of normal
liver health, most commonly due to bone disease or pregnancy.
GGT is induced by alcohol and other drugs and so lacks specificity for
many liver diseases.
Bilirubin ↑ es with increasing severity of liver disease.
In cases of ↑ed bilirubin or clinical jaundice, we should consider
haemolysis (Hb breaks down to form bilirubin. Lipid-soluble,
unconjugated bilirubin is conjugated in the liver, making it water-
soluble, and then excreted into bile).
ALT > AST (viral hepatitis); AST > ALT (alcoholic liver disease);
17.
Imp. Pointers (contd’.)
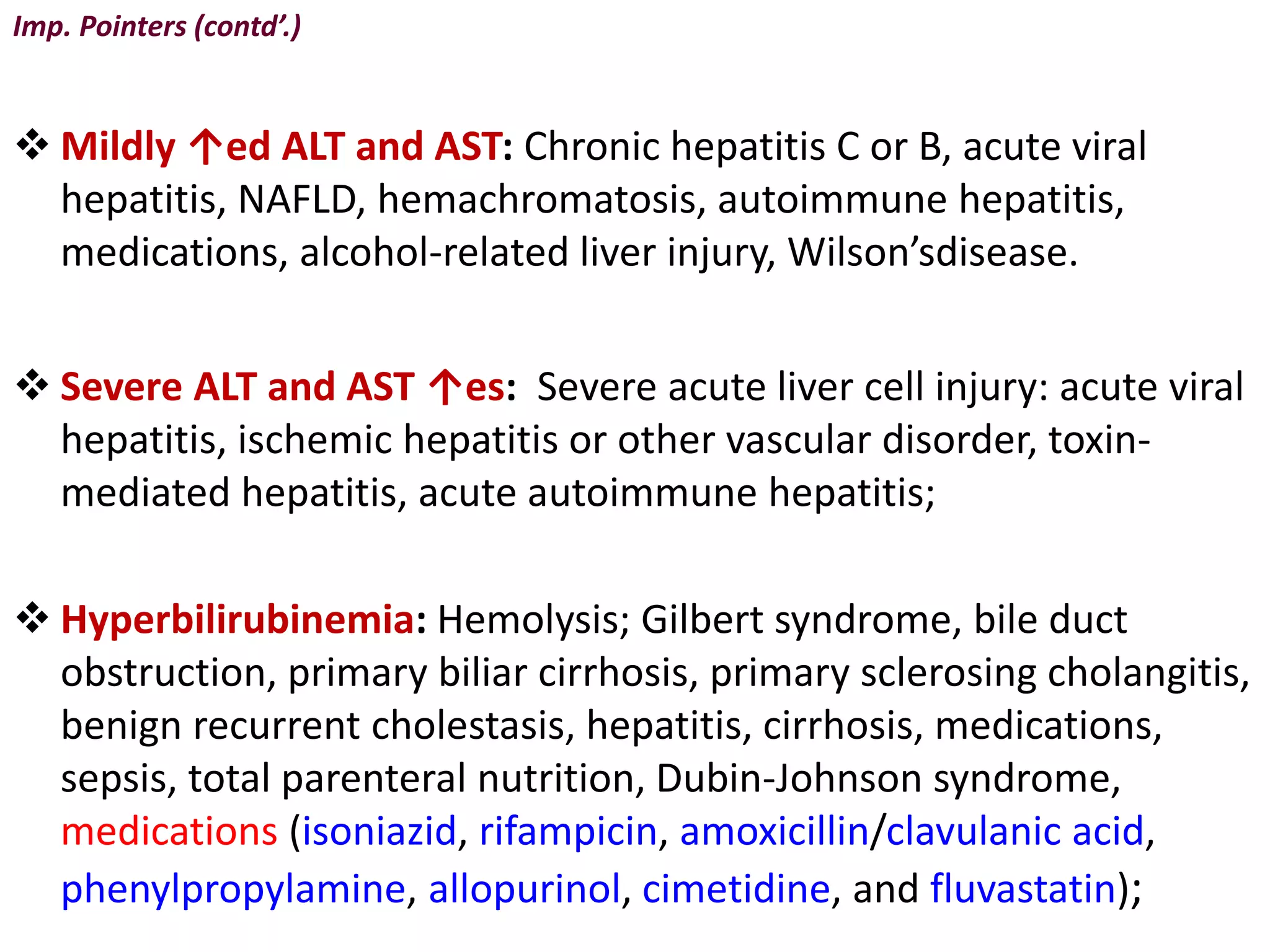
Mildly ↑ed ALT and AST: Chronic hepatitis C or B, acute viral
hepatitis, NAFLD, hemachromatosis, autoimmune hepatitis,
medications, alcohol-related liver injury, Wilson’sdisease.
Severe ALT and AST ↑es: Severe acute liver cell injury: acute viral
hepatitis, ischemic hepatitis or other vascular disorder, toxin-
mediated hepatitis, acute autoimmune hepatitis;
Hyperbilirubinemia: Hemolysis; Gilbert syndrome, bile duct
obstruction, primary biliar cirrhosis, primary sclerosing cholangitis,
benign recurrent cholestasis, hepatitis, cirrhosis, medications,
sepsis, total parenteral nutrition, Dubin-Johnson syndrome,
medications (isoniazid, rifampicin, amoxicillin/clavulanic acid,
phenylpropylamine, allopurinol, cimetidine, and fluvastatin);
18.
Imp. Pointers (contd’.)
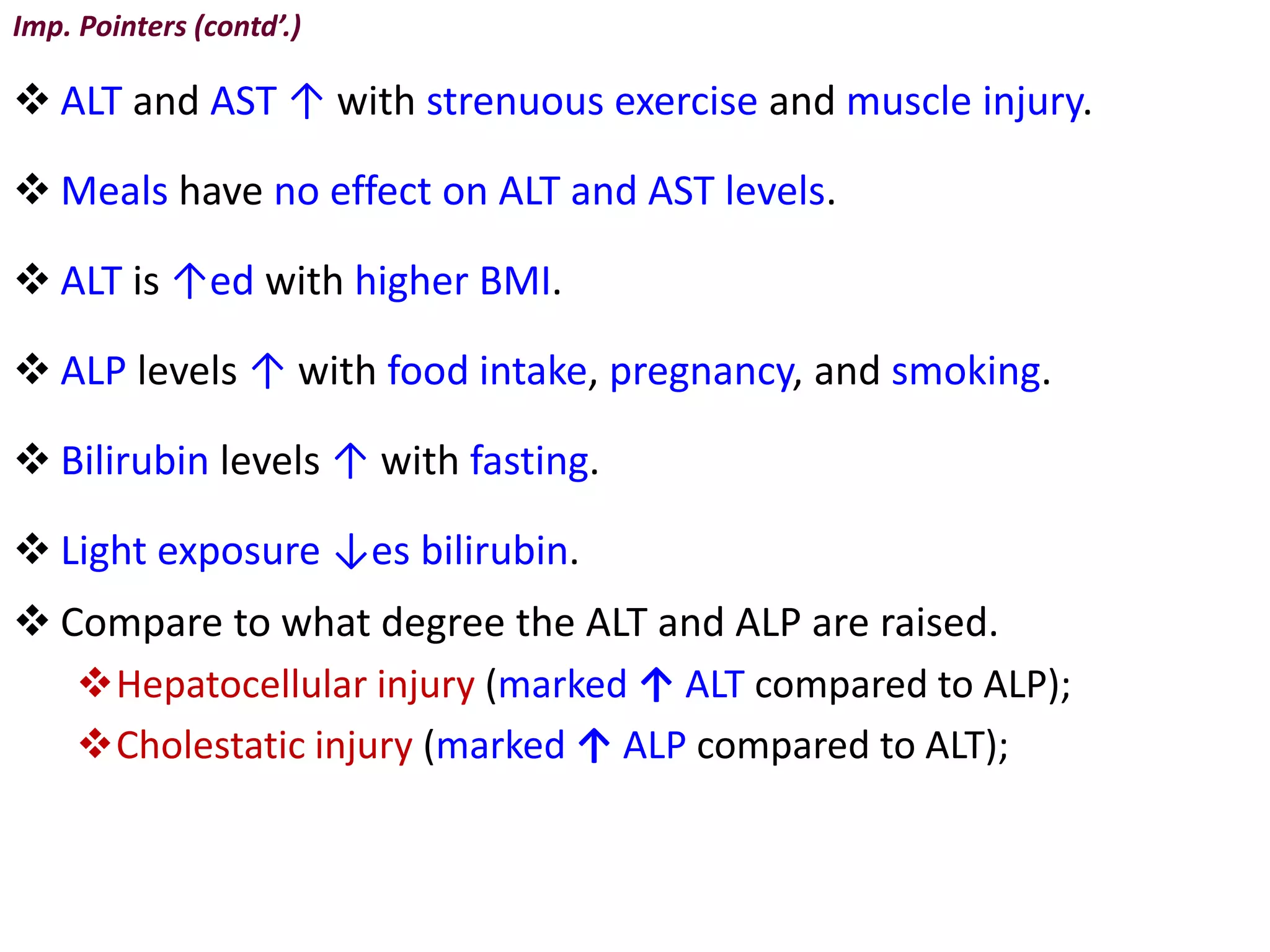
ALT and AST ↑ with strenuous exercise and muscle injury.
Meals have no effect on ALT and AST levels.
ALT is ↑ed with higher BMI.
ALP levels ↑ with food intake, pregnancy, and smoking.
Bilirubin levels ↑ with fasting.
Light exposure ↓es bilirubin.
Compare to what degree the ALT and ALP are raised.
Hepatocellular injury (marked ↑ ALT compared to ALP);
Cholestatic injury (marked ↑ ALP compared to ALT);
19.
Imp. Pointers (contd’.)
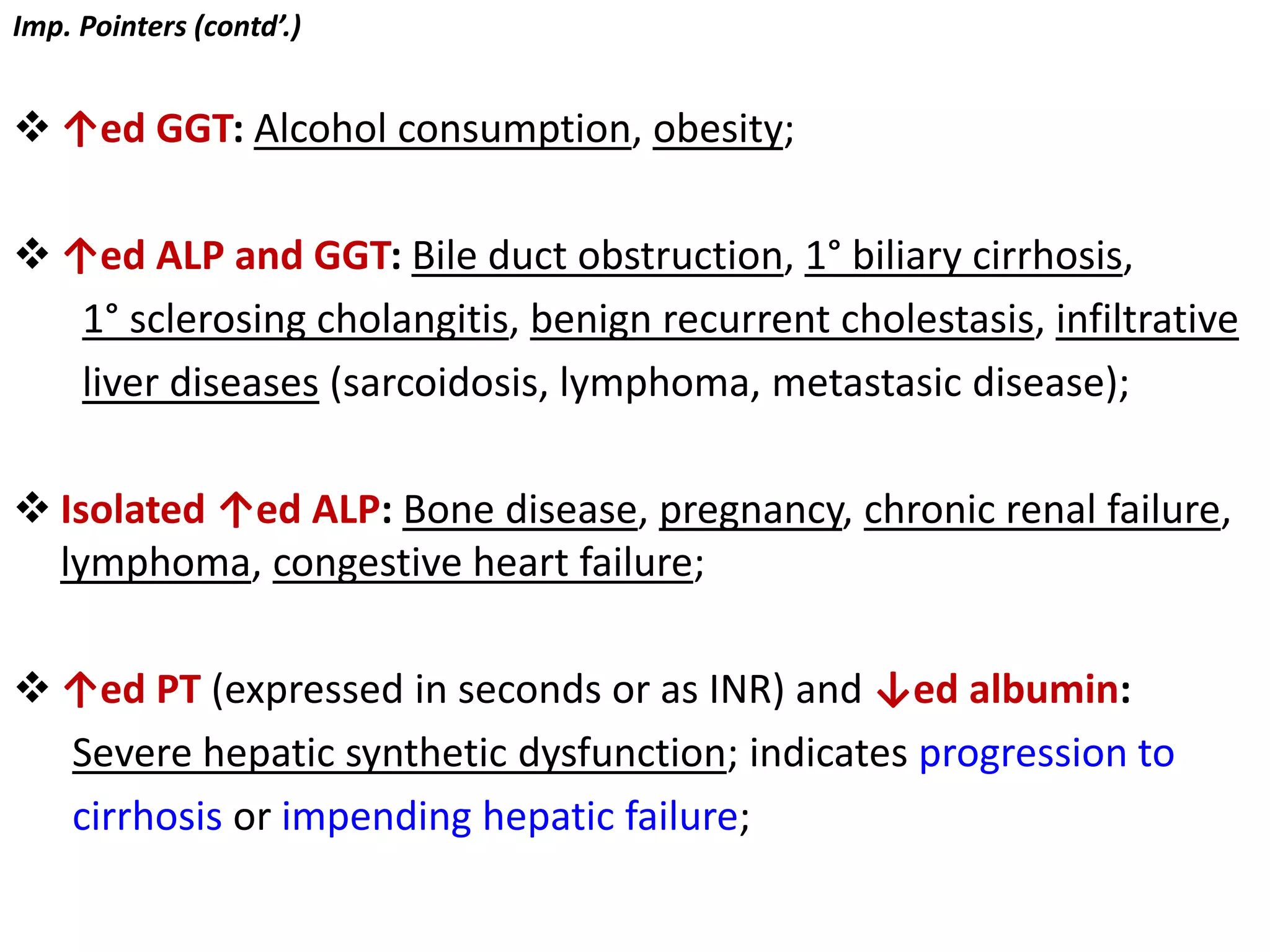
↑ed GGT: Alcohol consumption, obesity;
↑ed ALP and GGT: Bile duct obstruction, 1° biliary cirrhosis,
1° sclerosing cholangitis, benign recurrent cholestasis, infiltrative
liver diseases (sarcoidosis, lymphoma, metastasic disease);
Isolated ↑ed ALP: Bone disease, pregnancy, chronic renal failure,
lymphoma, congestive heart failure;
↑ed PT (expressed in seconds or as INR) and ↓ed albumin:
Severe hepatic synthetic dysfunction; indicates progression to
cirrhosis or impending hepatic failure;
20.
PT, Clotting factors,Vit.K
The PT is dependent on clotting factors’ activity.
Clotting factors are produced by the liver.
Production of clotting factors is dependent on adequate vit.K.
Clotting may also be prolonged by vitamin K deficiency.
PT is a good indicator of liver function (acute and chronic cases) if
vit.K levels are normal and in absence of anticoagulants usage(e.g.
warfarin).
International Normalized Ratio (INR)
The INR also reflects clotting and liver synthetic function.
INR is standardized across all laboratories in the world.
Liver function must be quite severely impaired to affect PT or INR.
Mild liver disease will most likely have normal values of PT and
INR.
21.
Always consider hemolysisif the serum bilirubin
levels are elevated.
• In cases of ↑ed bilirubin or clinical jaundice, we
should consider haemolysis (Hb breaks down to
form bilirubin. Lipid-soluble, unconjugated bilirubin
is conjugated in the liver, making it water-soluble,
and then excreted into bile).
![ Liver is the largest organ in the body (1.2-1.5 kgs.).
2 sources of blood supply to the liver:
• Hepatic artery (from the aorta; supplies O2-rich arterial blood);
• Portal veins (venous outflow of intestine and spleen);
Hepatic Function Tests (LFTs)
Most often used to determine:
• Presence and type of liver disease;
• Extent and progression of liver disease;
LFTs analyze:
1] Test of excretion by the liver
Reported as:
• Total Bilirubin [ Unconjugated (Indirect) + Conjugated (Direct)]
• Direct Bilirubin (Conjugated)](https://image.slidesharecdn.com/interpretationofhepaticfunctiontests-230522002047-bc8ab1c0/75/INTERPRETATION-OF-HEPATIC-FUNCTION-TESTS-pdf-2-2048.jpg)
![2] Evaluation of synthesis in
the liver
Albumin
Pre-albumin
Globulin
Total Protein
Prothrombin time
Cholesterol & esters
3] Enzyme activity evaluation
Serum transaminases
* AST (SGOT)
* ALT (SGPT)
Serum alkaline phosphatase
[ALP]
Lactate Dehydrogenase
[LDH]
ɣ-glutamyl transpeptidase
[GGTP]](https://image.slidesharecdn.com/interpretationofhepaticfunctiontests-230522002047-bc8ab1c0/75/INTERPRETATION-OF-HEPATIC-FUNCTION-TESTS-pdf-3-2048.jpg)
![ > 10x ↑ in ALT and < 3x ↑ in ALP (predominantly hepatocellular
injury);
[E.g., viral hepatitis, metabolic liver diseases, drug or alcohol
toxicity and autoimmune hepatitis]
< 10x ↑ in ALT and > 3x ↑ in ALP (cholestasis);
[E.g., Bile stones, cholestatic drug-induced liver injury]
It is possible for patients to have both hepatocellular injury and
cholestasis.](https://image.slidesharecdn.com/interpretationofhepaticfunctiontests-230522002047-bc8ab1c0/75/INTERPRETATION-OF-HEPATIC-FUNCTION-TESTS-pdf-9-2048.jpg)






















































![PHARMACOTHERAPY POINTERS FOR ATHEROSCLEROSIS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforatherosclerosismalaysiancpgs-230519014441-00a85dfd-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR SCHIZOPHRENIA [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforschizophreniamalaysiancpgs-230519020539-71314b89-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR ISCHEMIC STROKE [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforischemicstrokemalaysiancpgs-230519035129-300dc0e5-thumbnail.jpg?width=640&height=640&fit=bounds)
![Interpretation of Clinical Lab Data [CARDIAC] for newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatacardiacfornewbies-230518071258-e33c3626-thumbnail.jpg?width=640&height=640&fit=bounds)
![TDM POINTERS [GERIATIC & PAEDIATRIC PATIENTS].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/tdmpointersgeriaticpaediatricpatients-230518044517-7b716179-thumbnail.jpg?width=640&height=640&fit=bounds)
![Interpretation of Clinical Lab Data [PFTs] for Newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatapftsfornewbies-230518072330-48aef17c-thumbnail.jpg?width=640&height=640&fit=bounds)



![PHARMACOTHERAPY POINTERS FOR ANXIETY & AFFECTIVE DISORDERS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforanxietyaffectivedisordersmalaysiancpgs-230519033737-7916c3bc-thumbnail.jpg?width=640&height=640&fit=bounds)





















