Downloaded 286 times
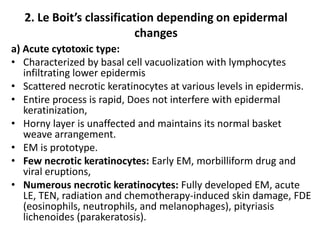
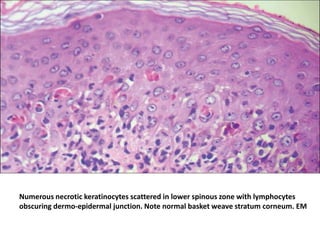
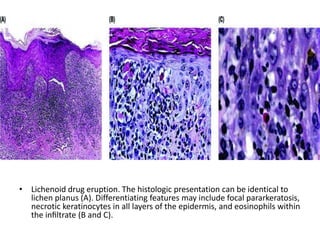
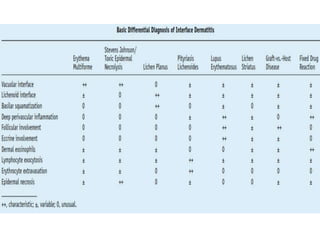

The document outlines the pathology and morphological characteristics of interface dermatitis, highlighting the role of T-cell-mediated damage at the dermal-epidermal junction. It describes the primary and secondary changes, including basal cell vacuolization and apoptotic keratinocytes, and classifies different types of interface dermatitis based on histological features and inflammatory patterns. Various conditions associated with interface dermatitis, including lupus erythematosus and lichen planus, are also discussed in relation to their specific histopathological findings.























































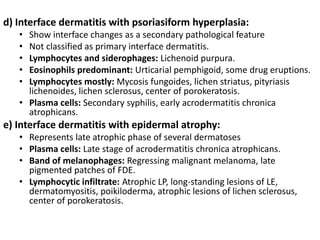
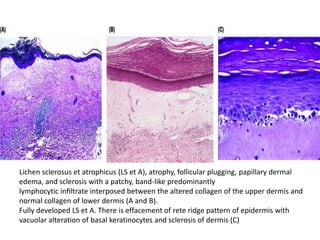
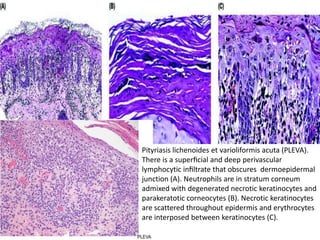
![Linear_Lesions_In_Dermatology [1].pptxhhh](https://cdn.slidesharecdn.com/ss_thumbnails/linearlesionsindermatology1-251122025615-0177ddce-thumbnail.jpg?width=640&height=640&fit=bounds)



















































