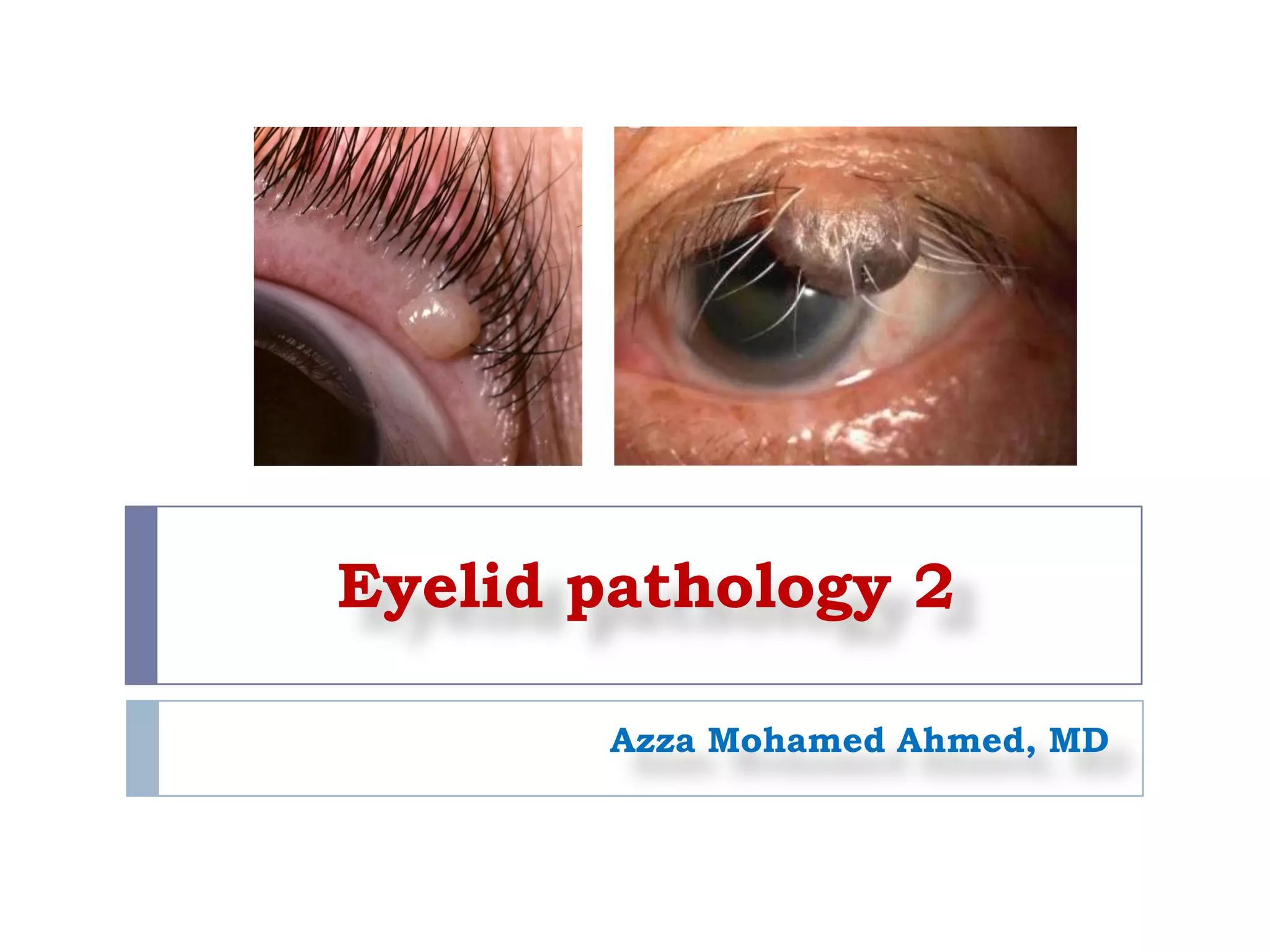
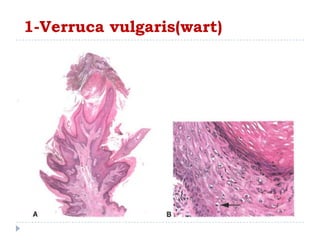
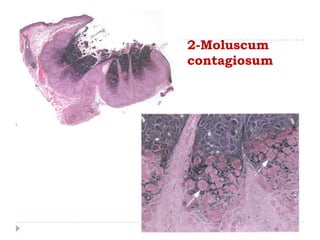
1. Viral infections like verruca vulgaris (wart) caused by human papillomavirus and moluscum contagiosum caused by poxvirus can infect the eyelid. Warts clinically appear as elevated papillary lesions and moluscum contagiosum appear as dome-shaped waxy nodules.
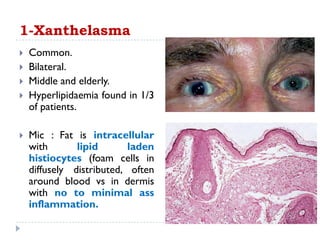
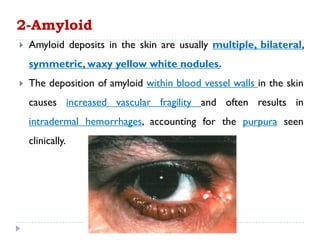
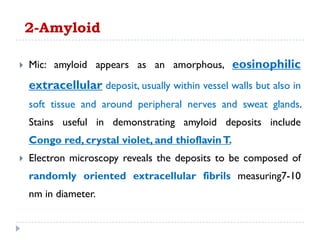
2. Degenerative diseases like xanthelasma and amyloidosis can affect the eyelid. Xanthelasma clinically appears as bilateral yellow plaques on the eyelids and amyloid deposits appear as multiple waxy nodules.
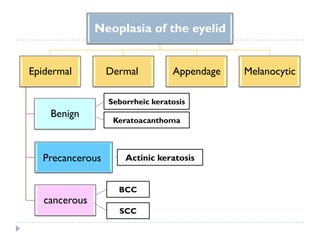
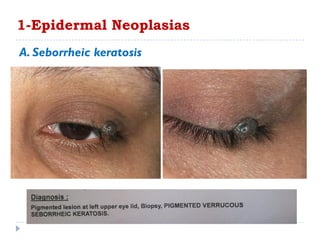
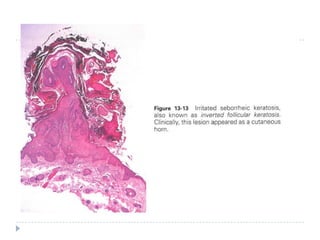
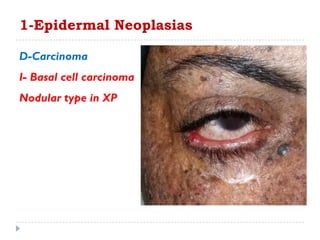
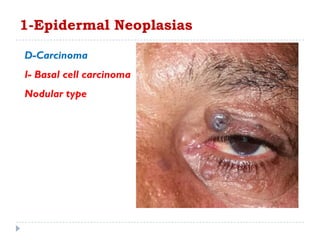
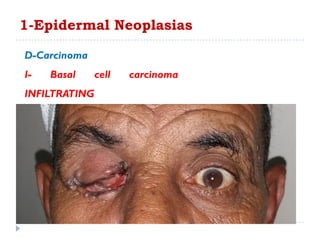
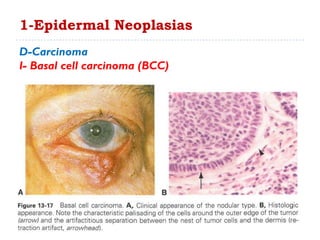
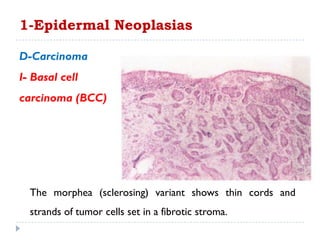
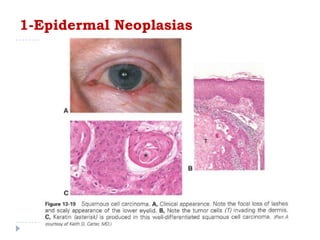
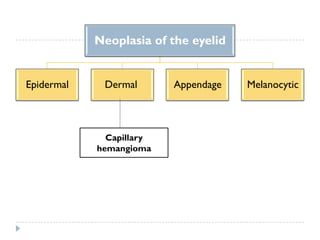
3. Various neoplasms can occur in the eyelid including seborrheic keratosis, basal cell carcinoma, squamous


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





