Downloaded 688 times











![Pathogenesis
A. INDUCTION PHASE
Self-peptides modified by exogenous antigens [viruses, medications
and contact allergens]) stimulation of keratinocytes and
plasmacytoid dendritic cells (pDCs), release IFN-α activation and
migration of DCs Ag presentation to naïve T-cells in lymph node
differentiation into CD8+ effector memory T cells attracted by
chemokines (released locally by pDCs) migrate into the inflammatory
site.](https://image.slidesharecdn.com/lichenoiddermatoses-141114183847-conversion-gate02/75/Lichenoid-dermatoses-potx-16-2048.jpg)












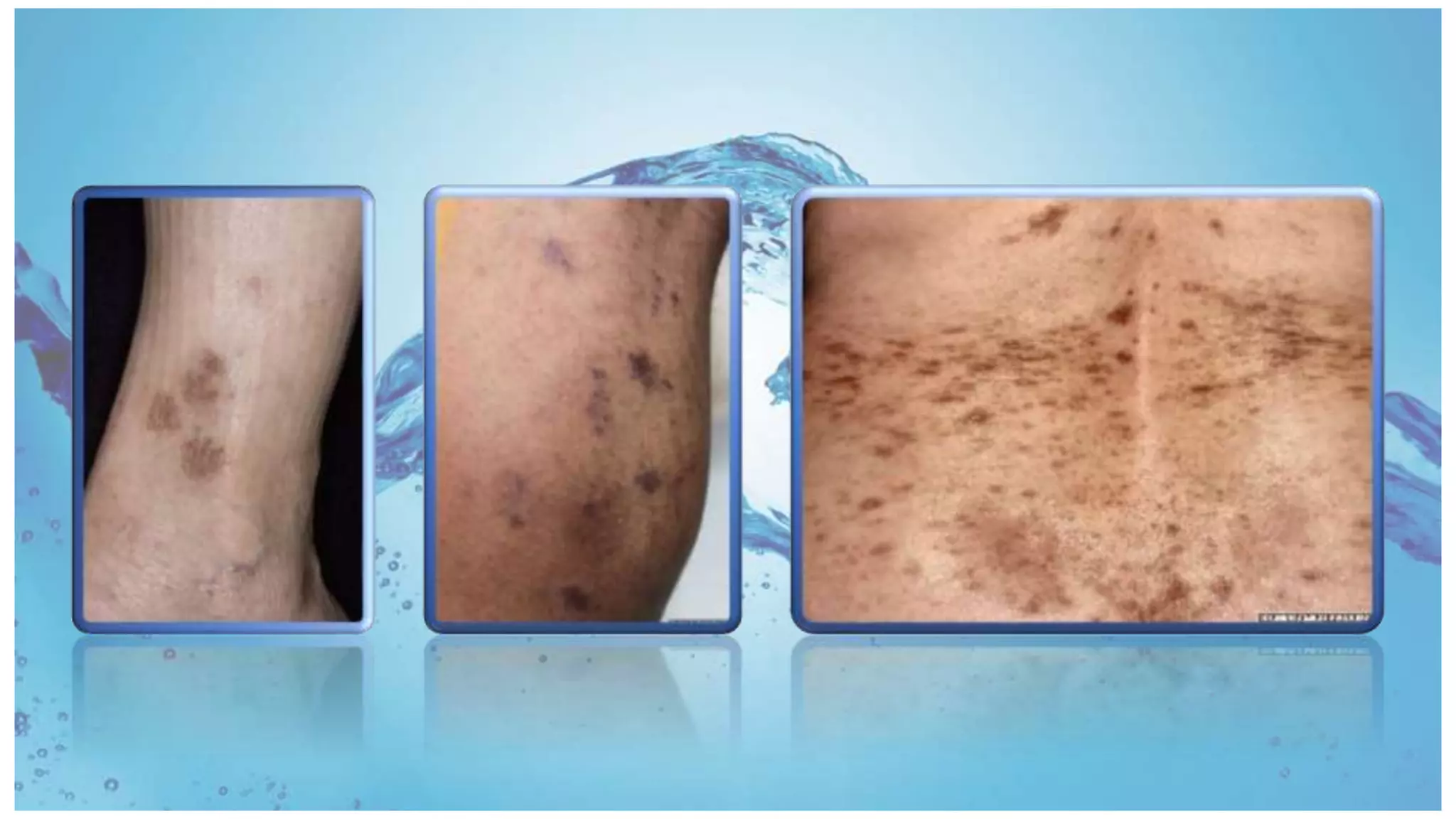





































































































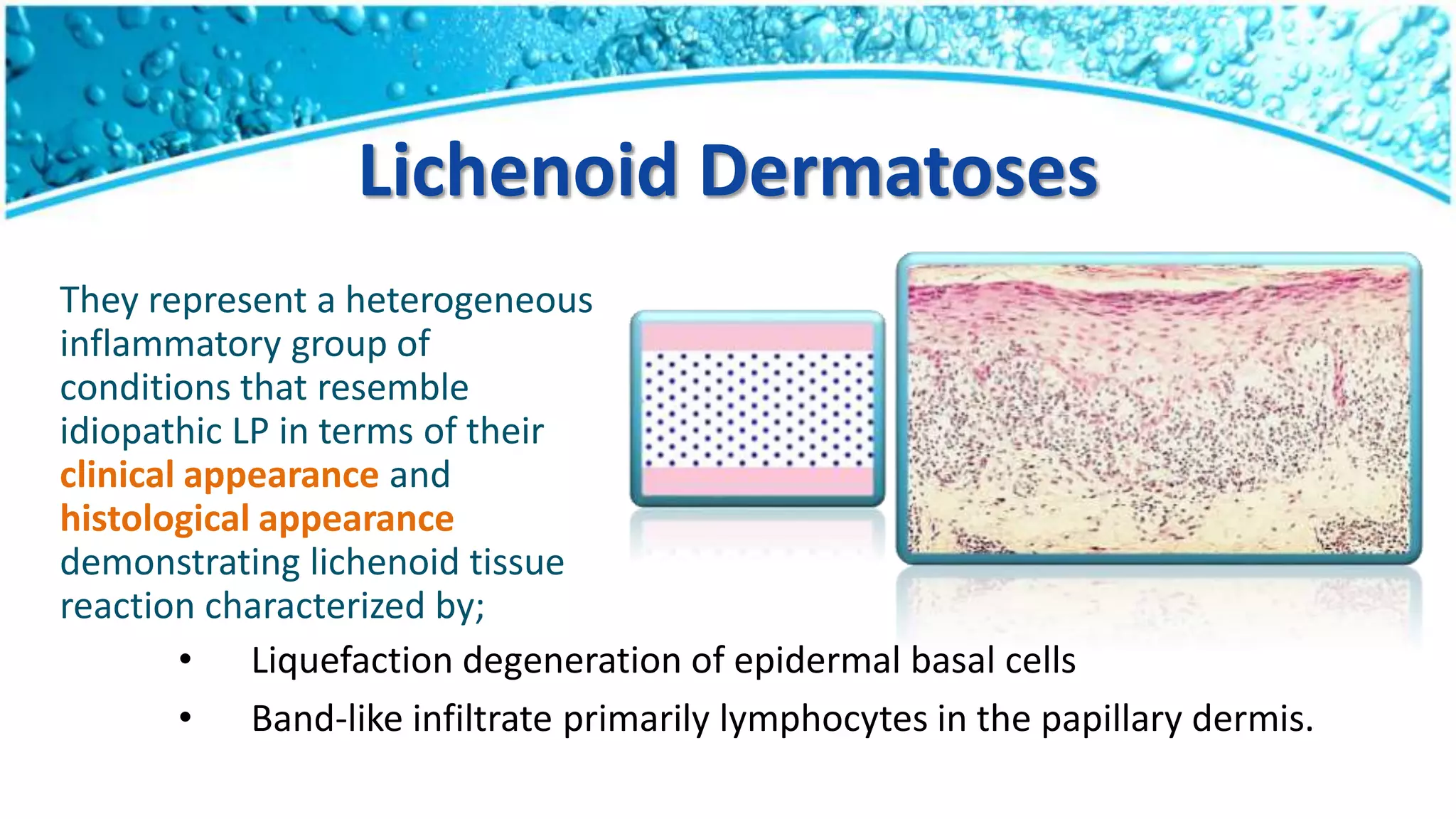
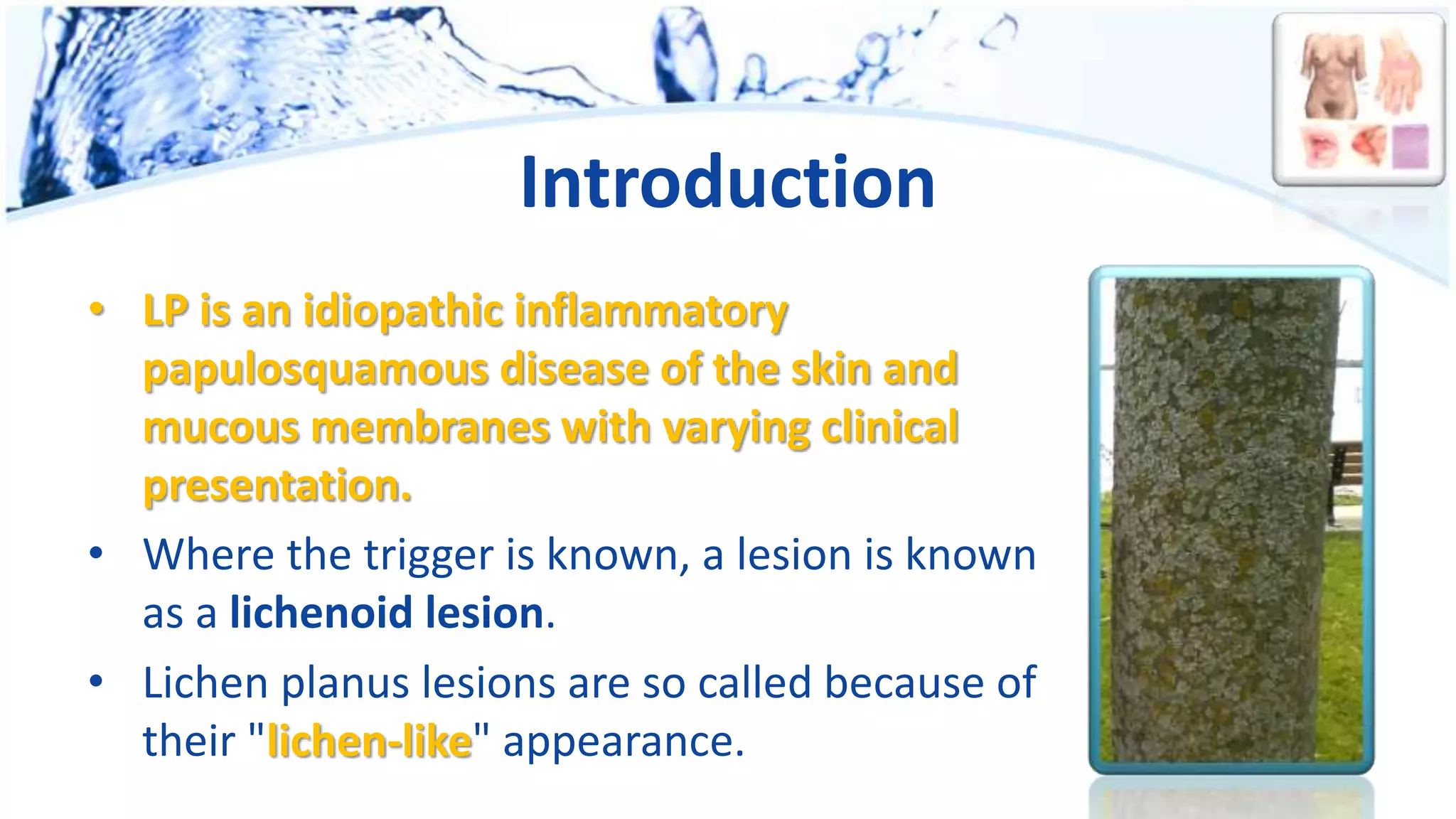
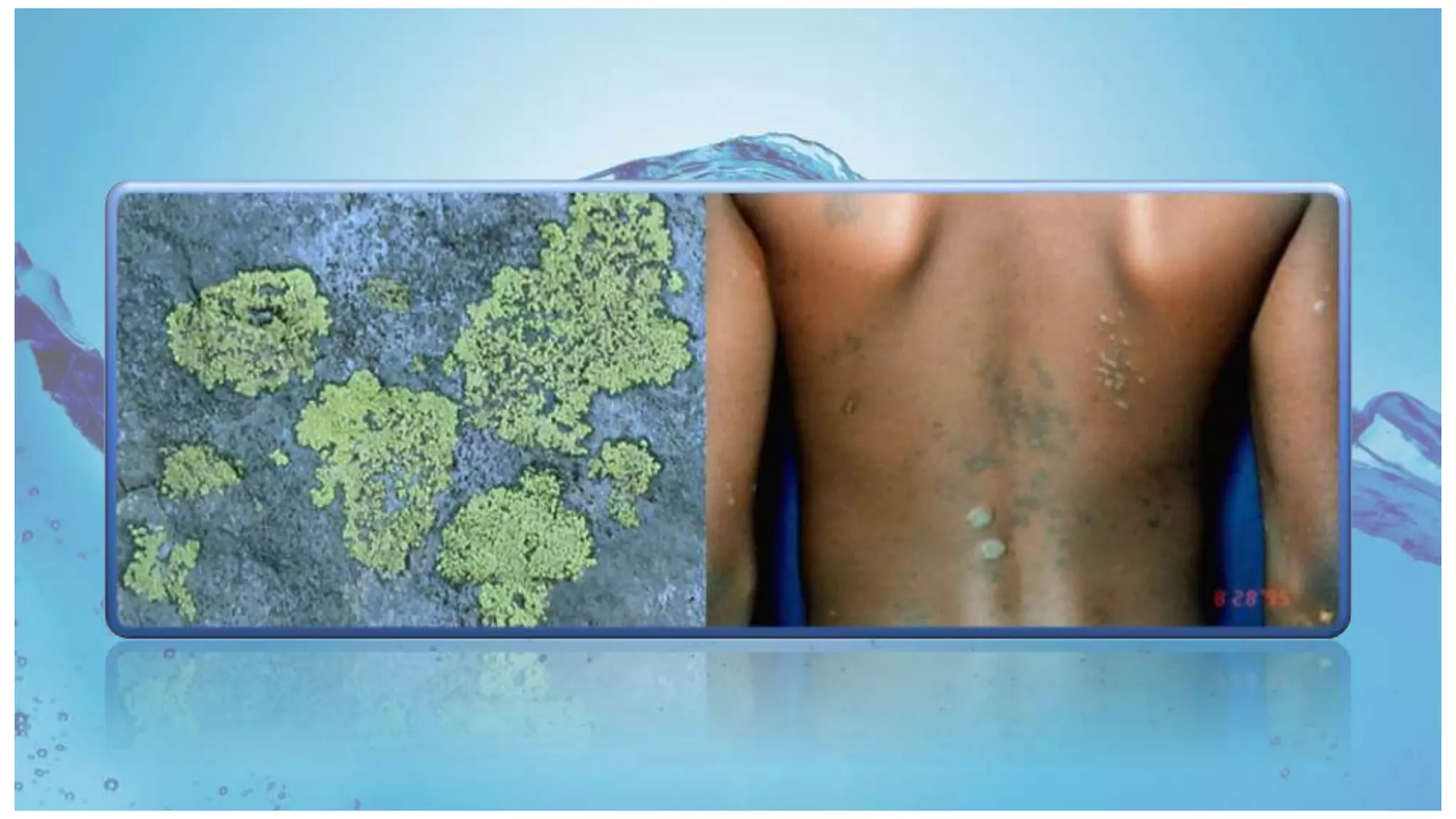
Lichenoid dermatoses are a diverse group of inflammatory conditions resembling lichen planus (LP) with distinct clinical and histological features, including liquefactive degeneration of epidermal basal cells and a lymphocytic band-like infiltrate. LP is characterized by its idiopathic nature, occurring mainly in adults with a prevalence of 0.2%-1% for cutaneous LP and 1%-4% for oral LP, often linked to autoimmune reactions, drug eruptions, and contact allergens. Variants of LP may manifest differently, including mucosal lesions and nail involvement, with potential chronic courses leading to serious complications such as scarring and malignancy.























































































