Downloaded 140 times
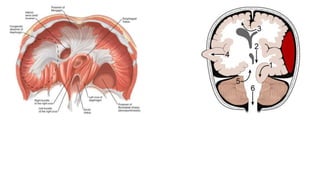
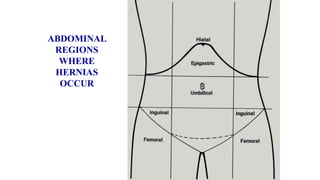


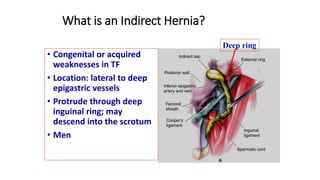
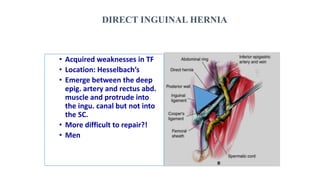













The document is a comprehensive overview of direct and indirect inguinal hernias, detailing their definitions, clinical features, and differences, along with associated complications. It describes the anatomy involved, types of hernia repairs, and surgical techniques such as Bassini and laparoscopic approaches. The objective is to educate students on understanding and managing inguinal hernias effectively.























































































