**Download to see my lecture notes!!**
Learn about the pathophysiology, clinical signs and symptoms, diagnosis and managment of the hernias of the groin- femoral and inguinal. Surgical approach is mentioned and common complications.
An epigastric hernia is where fat pushes out through a weakness in the wall of your abdomen between your umbilicus (belly button) and sternum and forms a lump
Femoral hernia is the third common hernia after inguinal and incisional hernias. The swelling in femoral hernia is below and lateral to pubic tubercle. It is more common in females. Strangulation is very common in this hernia.
Ventral hernia is protrusion of peritoneal sac through anterior abdominal wall defects except Groin hernias. In this presentation I have discussed Epigastric, Umbilical, Para umbilical, Incisional, Spigelian and Lumbar hernias.
An epigastric hernia is where fat pushes out through a weakness in the wall of your abdomen between your umbilicus (belly button) and sternum and forms a lump
Femoral hernia is the third common hernia after inguinal and incisional hernias. The swelling in femoral hernia is below and lateral to pubic tubercle. It is more common in females. Strangulation is very common in this hernia.
Ventral hernia is protrusion of peritoneal sac through anterior abdominal wall defects except Groin hernias. In this presentation I have discussed Epigastric, Umbilical, Para umbilical, Incisional, Spigelian and Lumbar hernias.
Simple notes on definition of abdominal hernias in general, as well as clinical features and management of inguinal hernias.
Brief explanation of hernia repair methods (laparoscopic, open surgery)
Inguinal and femoral hernia:
A hernia is a protusion of a viscus or a part of viscus through and abnormal opening in the walls of its containing cavity. Details of inguinal hernia and few slides on other types of hernia.
Simple notes on definition of abdominal hernias in general, as well as clinical features and management of inguinal hernias.
Brief explanation of hernia repair methods (laparoscopic, open surgery)
Inguinal and femoral hernia:
A hernia is a protusion of a viscus or a part of viscus through and abnormal opening in the walls of its containing cavity. Details of inguinal hernia and few slides on other types of hernia.
A hernia is the protrusion of an organ or the fascia of an organ through the wall of the cavity that normally contains it.There are different kinds of hernia, each requiring a specific management or treatment.
SIGNS AND SYMPTOMS
By far the most common hernias develop in the abdomen, when a weakness in the abdominal wall evolves into a localized hole, or "defect", through which adipose tissue, or abdominal organs covered with peritoneum, may protrude. Another common hernia involves the spinal discs and causes sciatica. A hiatal hernia occurs when the stomach protrudes into the mediastinum through the esophageal opening in the diaphragm.
Hernias may or may not present with either pain at the site, a visible or palpable lump, or in some cases more vague symptoms resulting from pressure on an organ which has become "stuck" in the hernia, sometimes leading to organ dysfunction. Fatty tissue usually enters a hernia first, but it may be followed or accompanied by an organ.
Hernias are not tears in the tissue but are openings in the adipose tissue. It is possible for a hernia to come and go, but in most cases a pain will persist.
Symptoms and signs vary depending on the type of hernia. Symptoms may or may not be present in some inguinal hernias. In the case of reducible hernias, a bulge in the groin or in another abdominal area can often be seen and felt. When standing, such a bulge becomes more obvious. Besides the bulge, other symptoms include pain in the groin that may also include a heavy or dragging sensation, and in men, there is sometimes pain and swelling in the scrotum around the testicular area.
Irreducible abdominal hernias or incarcerated hernias may be painful, but their most relevant symptom is that they cannot return to the abdominal cavity when pushed in. They may be chronic, although painless, and can lead to strangulation. Strangulated hernias are always painful and pain is followed by tenderness. Nausea, vomiting, or fever may occur in these cases due to bowel obstruction. Also, the hernia bulge in this case may turn red, purple or dark and pink.
In the diagnosis of abdominal hernias, imaging is the principal means of detecting internal diaphragmatic and other nonpalpable or unsuspected hernias. Multidetector CT (MDCT) can show with precision the anatomic site of the hernia sac, the contents of the sac, and any complications. MDCT also offers clear detail of the abdominal wall allowing wall hernias to be identified accurately.
CAUSES OF HERNIA
Causes of hiatal hernia vary depending on each individual. Among the multiple causes, however, are the mechanical causes which include: improper heavy weight lifting, hard coughing bouts, sharp blows to the abdomen, and incorrect posture.
Furthermore, conditions that increase the pressure of the abdominal cavity may also cause hernias or worsen the existing ones. Some examples would be: obesity, straining during a bowel movement or urination (constipation, enlarged prostate).
This is a case study done by me as a part of my in-service education progamme in my institution...hope this may help all nurses who wants to do a case study.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Acute scrotum is a general term referring to an emergency condition affecting the contents or the wall of the scrotum.
There are a number of conditions that present acutely, predominantly with pain and/or swelling
A careful and detailed history and examination, and in some cases, investigations allow differentiation between these diagnoses. A prompt diagnosis is essential as the patient may require urgent surgical intervention
Testicular torsion refers to twisting of the spermatic cord, causing ischaemia of the testicle.
Testicular torsion results from inadequate fixation of the testis to the tunica vaginalis producing ischemia from reduced arterial inflow and venous outflow obstruction.
The prevalence of testicular torsion in adult patients hospitalized with acute scrotal pain is approximately 25 to 50 percent
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
New Drug Discovery and Development .....NEHA GUPTA
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
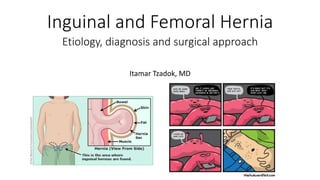
1. Inguinal and Femoral Hernia
Itamar Tzadok, MD
Etiology, diagnosis and surgical approach
2. Table of contents
• Definitions and general concepts.
• Hernias of the groin area.
• Inguinal hernia.
• Femoral hernia.
• Ventral hernias.
• Unusual hernias.
3. Components of hernia
• Hernia: abnormal protrusion of an organ or tissue through a defect in
its surrounding walls.
• Hernial defect (orifice).
• Neck of hernia.
• Sac of hernia.
• Hernial contents
4. Abdominal wall hernias
• Abdominal wall hernias occur only at sites
at which the aponeurosis and fascia are
not covered by striated muscle.
5. Modes and complications of hernia
• Reducible hernia.
• Irreducible hernia.
• Incarcerated hernia.
• Strangulated hernia.
6. Classification of hernias
• Internal / external.
• Region (groin, abdomen etc).
• Etiology:
• Congenital= The defect in the abdominal wall is present from birth.
• Acquired= development of defect.
7. Swelling in the groin area – DDX
• Anatomical / tissue sieve.
8. Inguinal hernia – surface anatomy
• Anterior superior iliac spine (ASIS).
• Pubic tubercle (PT).
• Inguinal ligament – PT-ASIS.
• Deep ring – midpoint of inguinal ligament.
• Superficial ring – medial and above PT.
11. Inguinal hernia – The Hesselbach triangle
• Direct inguinal hernias protrude
through the abdominal wall in this
region.
• Superior border- inferior epigastric a.
• Medial border- rectus abdominis.
• Inferior border- inguinal ligament.
14. Hernias of the groin – summary
• Inguinal hernia = a protrusion of abdominal-cavity contents through
the inguinal canal.
• Femoral hernia = a protrusion of abdominal-cavity contents through
the femoral canal .
Femoral herniaIndirect inguinal
hernia
Direct inguinal hernia
Femoral canalDeep inguinal ring.Inguinal canal
posterior wall.
Hesselbach triangle.
Sac of hernia
protrusion point
-Lateral.Medial.Sac of hernia location
relating to the inferior
epigastric artery
Inferior.Superior.Superior.Relation to inguinal
ligament (protrusion)
16. Groin hernia – epidemiology
• 96% of groin hernia are inguinal, 4% are femoral.
• Direct : Indirect = 1:2.
• Men are 25 times more likely to have groin hernia.
• Indirect inguinal hernia is the most common in both sexes.
• Femoral hernia- more common in women (yet inguinal hernias are
more common).
17. Groin hernia – epidemiology (cont.)
• History of hernia or prior hernia repair (including childhood)
• Older age
• Male sex
• Caucasian race
• Chronic cough
• Chronic constipation
• Abdominal wall injury and surgery
• Smoking
• Family history of hernia
• Straining to void urine
• Heavy lifting
• Obesity
19. Groin hernia – history taking
• Age.
• Occupation.
• Local symptoms – painless swelling, groin pain without swelling.
• Other abdominal symptoms – change in bowel habits.
• Bowel obstruction cardinal – if obstructed hernia.
• Family history of hernias.
• Past surgeries.
Ask about risk factors – influence strength of abdominal wall or
increase intra abdominal pressure.
20. Inguinal hernia – signs and symptoms
• Examine inguinal areas while patient stands up.
• Cough impulse.
• Ask patient to reduce hernia.
• Try to reduce hernia.
• Examine scrotum.
• Palpate external inguinal ring and look for budges
• Signs of compromised hernia content:
• Local skin changes- edema, erythema.
• Hard and tender hernia.
27. Results of surgical hernia repairs
• Open repairs can be performed under local anesthesia.
• Tension-free repairs have a lower rate of recurrence than tissue repairs.
• The laparoscopic repair resulted in a more rapid return to normal activity and decreased
persistent postoperative pain.
• Open and laparoscopic mesh repairs had similar recurrence rates.
• TAPP (compared to TEP) procedures were associated with more port site hernias and
vascular injuries.
• TEP (compared to TAPP)approach had a greater conversion rate.
28. Inguinal hernia repair - complications
• Perioperative complication
• Bruising, seroma, and hematoma formation (common)
• Bladder injury (rare)
• Later complications
• Persistent groin pain and post-herniorraphy neuralgia
(common).
• Testicular complications.
• Deep wound/mesh infection.
• Recurrent hernia.
• Mesh migration and erosion – primary/secondary.
29. Ventral hernias
• Definition = protrusion through the anterior abdominal wall fascia.
• Spontaneous / acquired.
• Acquired = incisional hernias.
• Location on the abdominal wall.
• Umbilical hernia.
• Epigastric hernia.
30. Unusual hernias
• Definition = hernias that occur infrequently. Classified according to
location on the abdominal wall.
• Spigelian hernia.
• Obturator hernia.
• Lumbar hernia.
• Interparietal hernia.
• Sciatic hernia.
• Perineal hernia.
• Loss of domain hernia.
31. Recap
• The components of the hernia (sac, neck, content).
• Classifications – region, etiology.
• Groin hernias – femoral and inguinal.
• Repairing inguinal hernia.
• Other uncommon hernia.
32. References
• Sabiston Textbook of Surgery, 20th ed.
• Browse’s Symptoms & Signs of Surgical Disease, 5th ed.
• Oxford Handbook of Clinical Medicine, 9th ed.
• Essentials of general surgery, 5th ed.
• Surgical Talk, 2nd ed.
• Up-To-Date.
33. Thank you!
Do you like this presentation?
Please let me know- like, share and follow
Editor's Notes
This presentation concers inguinal hernia- anatomy, clinical evaluation, classifications, surgical technique and common operative complications.
We will put empheisis on the differences between inguinal and femoral hernias.
There are other hernias- but we will only mention high yield facts regarding them.
A hernia might happen everywhere in the human body (for example- herniation of the brain)
An abdominal hernia is happening when an element of the abdomanial space is protruding through a defect in the a abdominal wall
The Sac of the hernia= A bag made of peritoneum
The neck of the hernia= The part of the hernia sac that is in contact with the abdominal wall defect.
Hernial content= the organs or tissue that fills the sac. For example- intestinal loop, colon or omental fat.
The fundus of the sac= the widest part of the hernia sac
Picture is from: http://www.surgwiki.com/wiki/Hernias
Sabiston Textbook of Surgery, 20th ed- page 1117.
An abdominal wall hernia will happen in an areas of mechanical weakness. Where the weight bearing element of the wall is afascia or aponeurosis, and there is no muscle element that contributes to the mechanical strength.
Illustrations from- Browse’s Symptoms & Signs of Surgical Disease , page 465.
Reducible= the hernia can be reduced back to it’s place.
Irreducibility= the hernia can’t be reduced (can’t be putted back) into the abdominal space.
Incarceration= the hernias’ content is attached to the sac and therefore can’t be reduced.
Strangulation= the contents of the hernia sac blood supply is cut off. Clinically- this is the stage where the patient is in pain and needs a surgical intervention.
Hernias can be classified in many ways.
Internal vs External:
Internal hernia= takes place between internal compartments of the body. For example- cerebral herniation, hiatal hernia.
External hernia= from an internal compartment, to an outer compartment. For example- inguinal hernia, ventral hernia.
Regional classification- we will focus on the inguinal area.
Etiological classification- Congenital vs acquired
Acquired- any condition that cause a repetitive increase of intra-abdominal pressure (coughing, heavy lifting) or conditions that reduce the mechanical strength of the abdominal wall (aging, post-surgical scarring)
Swelling in the groin is not always a sign for an inguinal hernia..
One way to approach the differential diagnosis (DDX) is using the anatomical sieve as presented in the book Surgical Talk, page 22.
Inguinal hernia and femoral hernia are the most common types of hernias and we will focus on them from here on.
Illustration from: http://geekymedics.com/hernias-explained/
Another image from Browse’s Symptoms & Signs of Surgical Disease page460.
http://geekymedics.com/hernias-explained/
Image taken from Oxford Handbook of Clinical Medicine page 617.
Inguinal hernia is classified by its relations with the epigastric artery- as direct (medial to the artery) or indirect (lateral to the artery)
Let’s recap- there are two types of hernias that develop in the area of the groin- femoral and inguinal hernias. Inguinal hernias are divided to direct and indirect.
The surgical approach to femoral and inguinal hernia is different- therefore we should know how to distinguish between them.
It is less important to tell the differences between direct and indirect inguinal hernia- because surgical management is similar.
An image from the book “essentials of general surgery”, as another recap and comparison
According to Sabiston
According to uptodate
Nyhus classification regards inguinal hernias.
Image from “Bates” page 521
Ask the patient- is the hernia constant, or appears in certain occasions?
Does the hernia reduces spontaneously or reduced after a manipulation?
Ask the patient to reduce the hernia. View it from different angles.
Surgery is not the only treatment. Sometimes the risk is greater than the benefit.
Under watchful waiting- only a small amount of hernias (0.3%) will incarcerate.
Non-operative treatment such as trusses/belts might improve symptoms, but still has risk for complications.
The definitive treatment for hernia is surgery- open access or minimally invasive (laparoscopic)
The repair of the defect which causes the hernia can be done using a tissue (also called tissue repair, tension repair)
Or can be done using a synthetic mesh (also called tension free repair)
The surgery can be classified according to the location on which the repairing element (tissue/mesh) is placed- anterior or posterior to the transversalis fascia.
The anatomical structures that we must find during the surgery:
Arcuate line: deep to the line, the transversalis fascia is the only component of the posterior part of the rectus sheath
The relative location of the peritoneum
Anterior approach- the mesh is placed anteriorly to the transversalis fascia
Preperitoneal approach- the mesh is placed posteriorly to the transversalis fascia
TEP = the mesh is laid superficially to the peritoneum. Therefore, the risk for adhesions is lower because the peritoneum is not dissected.
TAPP= the mesh is laid deep to the peritoneum.
Conversion rate= how many minimally invasive procedures change into open procedure, after starting the operation.
The most interesting outcome regarding hernia repair surgeries is recurrence of the hernia.
A recurrence in a patient that underwent an open repair=> the next procedure will be laparoscopic repair.
A recurrence in a patient that underwent a laparoscopic repair=> the next procedure will be an open repair.
Perioperative complications are defined as complications that arise since the beginning of hospitalization until the recovery from the surgery:
Bruising= the most common complication. Can be reduced by good surgical technique. Minimizing retraction.
Seroma, hematoma= a collection of body fluid in the space that was left after reducing the hernia. It is usually self limited, and there is no need for drainage unless there are signs of infection.
Bladder injury= in laparoscopic surgery, while placing a trocar
Later complications appear weeks and even years after the procedure.
Persistent groin pain- a pain that persists for more than 3 months after surgery
Testicular complications- testicular pain, ischemic orchitis, and testicular atrophy. All might result if the spermatic cord is injured during the procedure
Mesh infection- might arise even years after procedure. The patient chief complaints will be fever, rigors, fatigue. The skin above the repair area will be warm, tender and painful.
Recurrent hernia- it depends on the surgical approach. Usually tension free (mesh repair) have lower hernia recurrence rates.
Mesh migration and erosion- can be primary and secondary. Primary= the mesh disconnects from neighboring tissues and starts to migrate in the path of least resistance. Secondary= the mesh is being rejected by the host and starts to migrate.
So far, we discussed hernias of the groin area (the common hernias).
Lets mention ventral hernias
Browse’s Symptoms & Signs page 458.
Less common hernias
Browse’s Symptoms & Signs page 458.