This document discusses infection control and reducing nosocomial infections. It defines key terms like infection control, nosocomial infections, disinfection and sterilization. It outlines the objectives of understanding infection control concepts and programs. It describes the epidemiology of common nosocomial infection sites and microorganisms. It explains the goals and functions of an infection control committee. It provides strategies to reduce nosocomial infections through hand hygiene, isolation protocols, ensuring clean environments, and sterilization of instruments. It emphasizes the importance of employee health programs and antimicrobial monitoring by the infection control committee and drug and therapeutics committee.

![Epidemiology of Nosocomial Infections
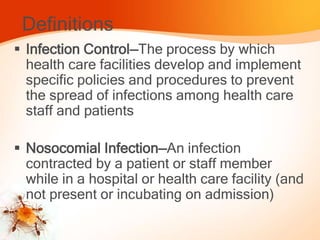
Most common sites for nosocomial infections
Surgical incisions
Urinary tract (i.e., catheter-related)
Lower respiratory tract
Bloodstream (i.e., catheter-related) Common microorganisms
Aerobic gram-positive cocci (Staphylococcus aureus,
enterococci [vancomycin-resistant]),
Aerobic gram-negative bacilli (Escherichia coli, P.
aeruginosa, Enterobacter spp., and Klebsiella
pneumoniae](https://image.slidesharecdn.com/infectioncontrolcommitte-copy-171207145701/85/Infection-control-comitte-7-320.jpg)





















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



