Downloaded 161 times

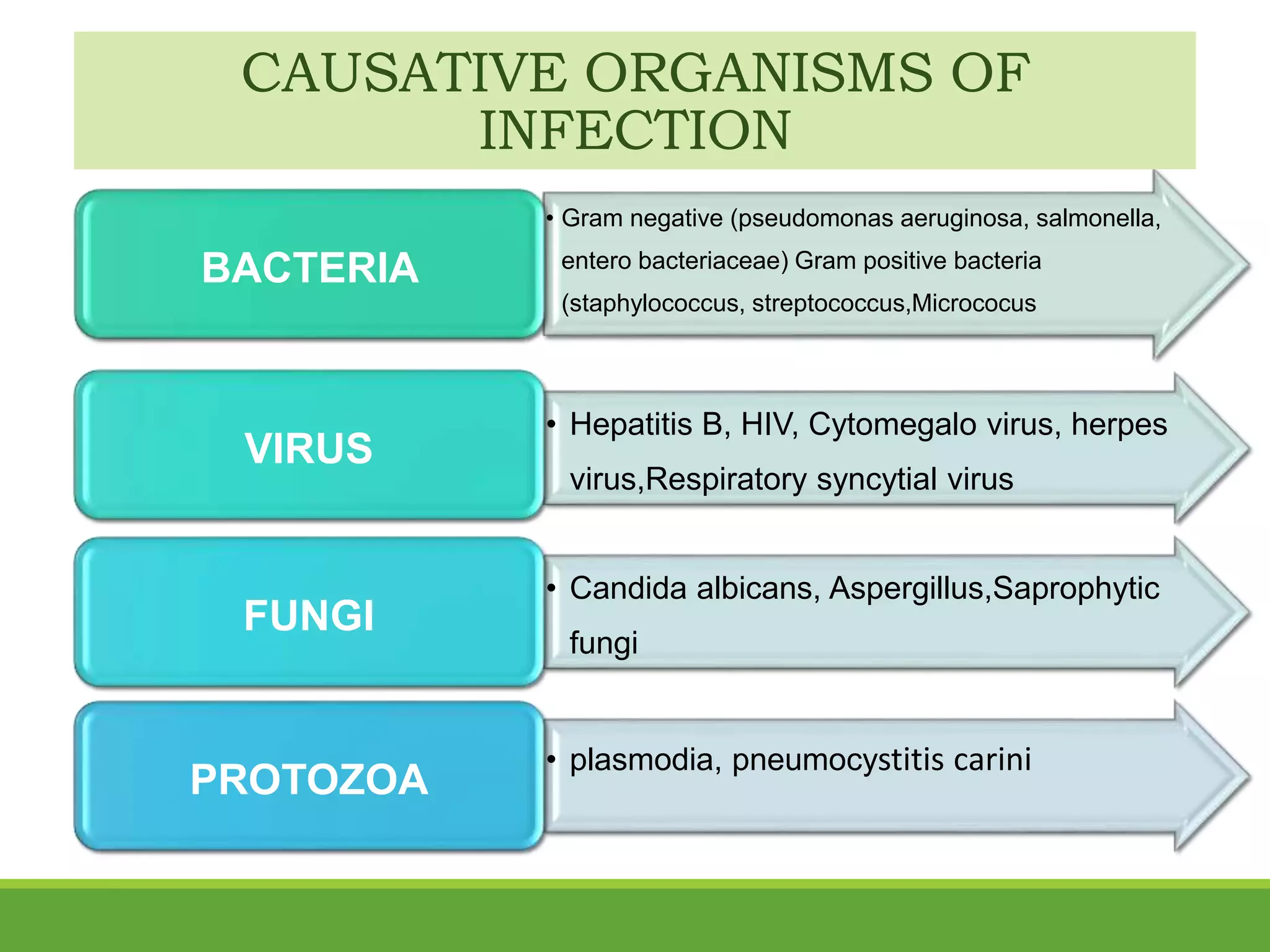


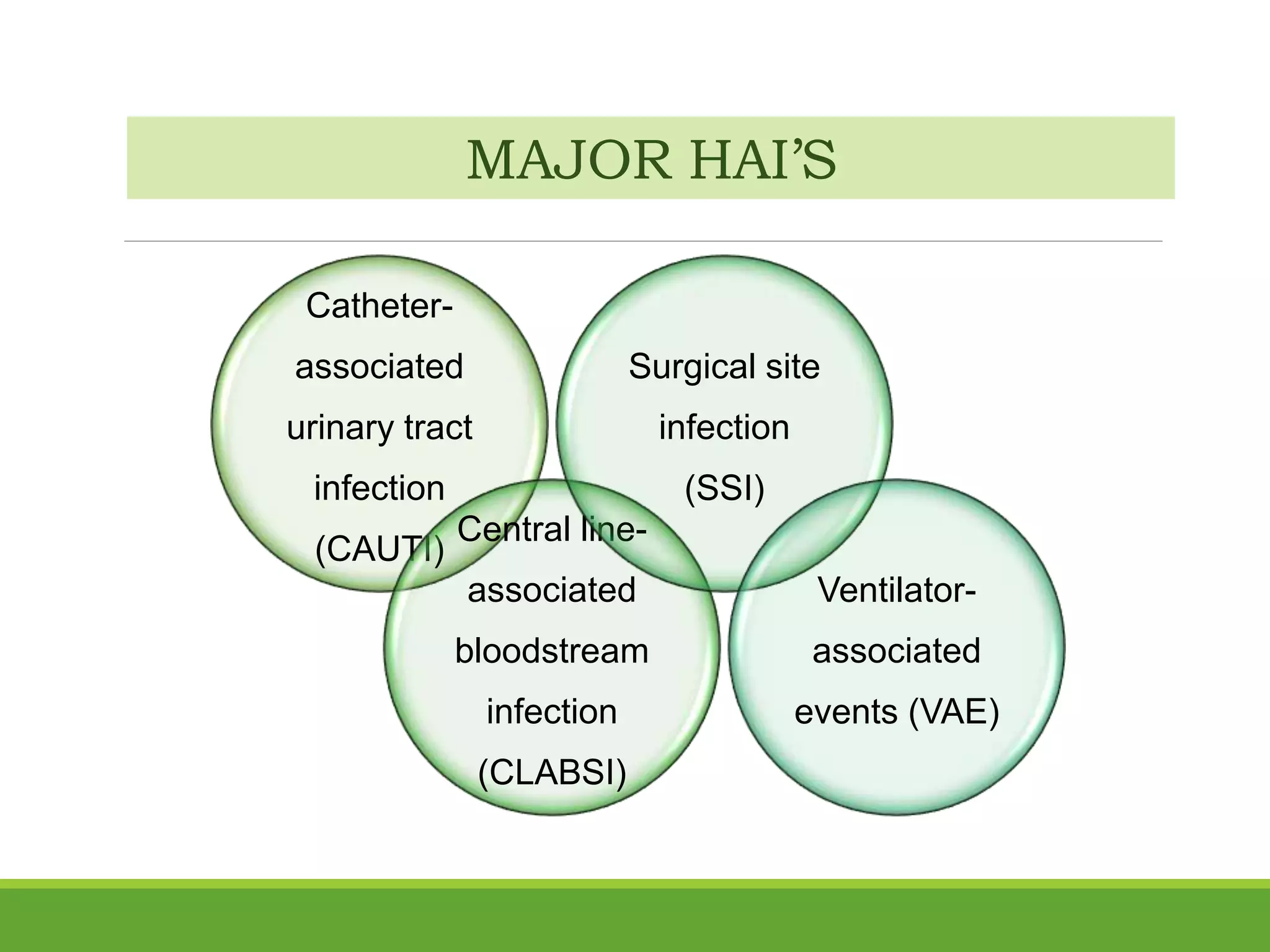
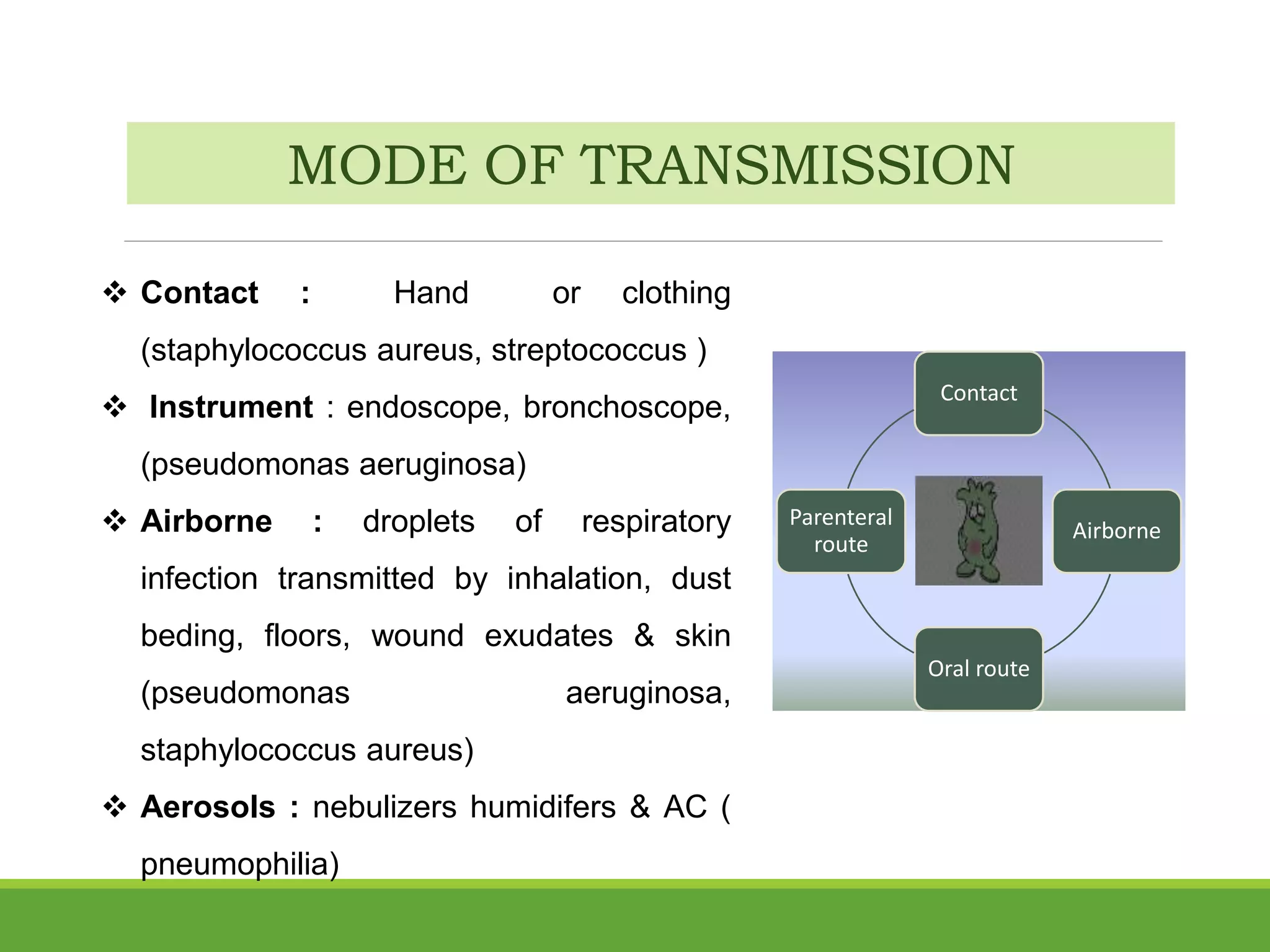



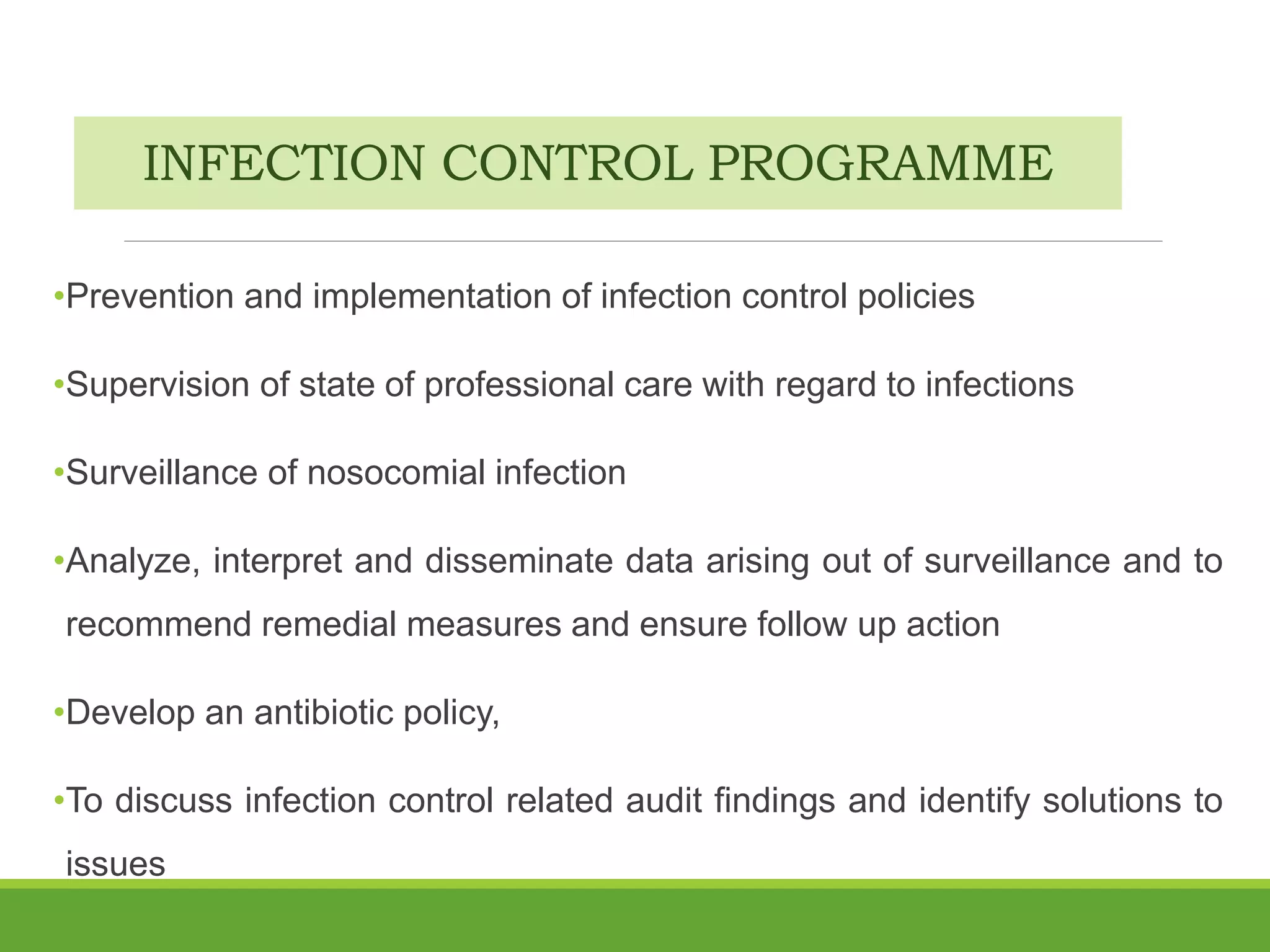



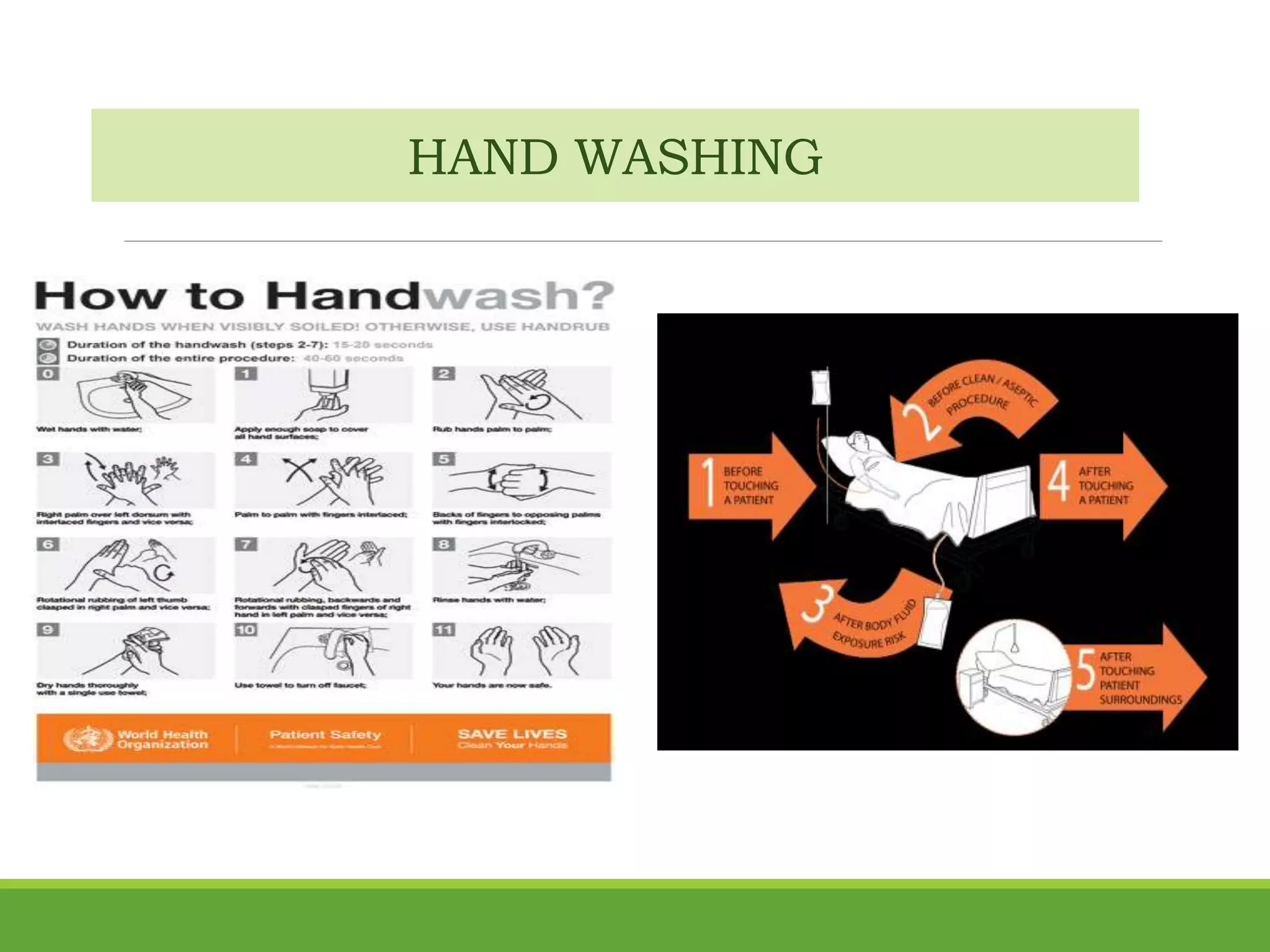


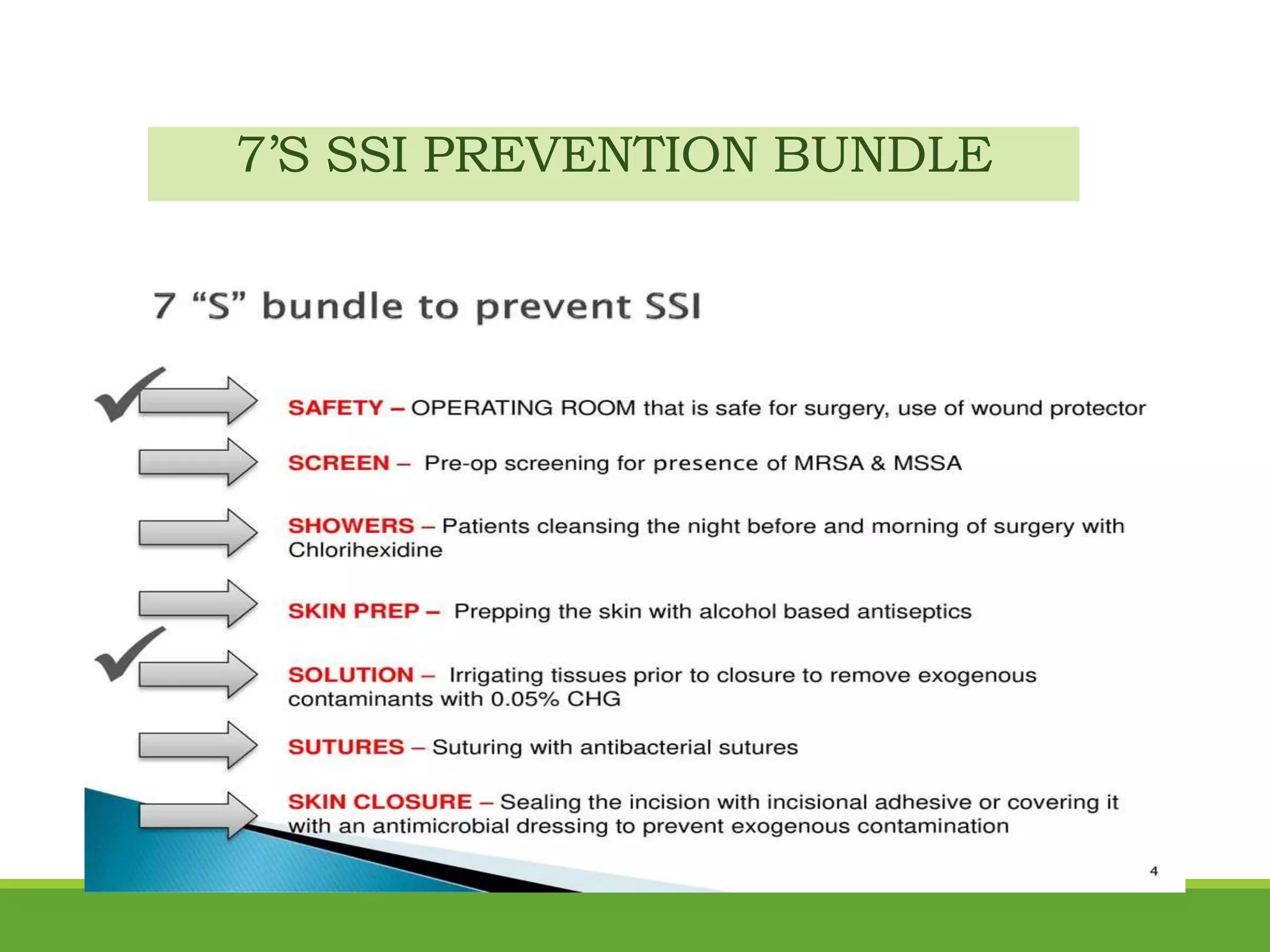








Nosocomial or hospital-acquired infections are a major problem, especially in intensive care units. The document discusses the definition, incidence, common types of infections, causative organisms, risk factors, modes of transmission, prevention methods, and the roles and responsibilities of nurses and infection control programs. It emphasizes the importance of hand hygiene, use of personal protective equipment, surveillance, policies, training, and guidelines to reduce infection rates in critical care units.































































![Human genome project [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/humangenomeprojectautosaved-210929062307-thumbnail.jpg?width=640&height=640&fit=bounds)






















