
Downloaded 158 times


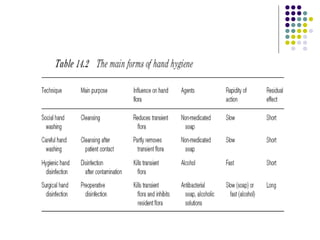
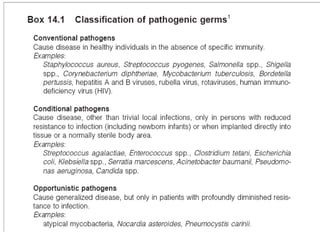
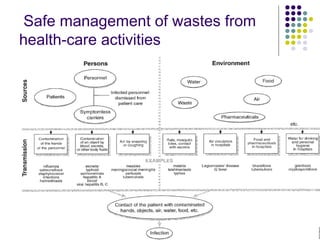
This document provides an overview of nosocomial infections, also known as hospital-acquired infections. It discusses what causes infections, the prevalence of hospital-acquired infections ranging from 3-25% depending on the hospital, and the two main forms of nosocomial infections - endogenous infections from an existing infection in the patient or cross-contamination from an external source in the hospital. It also outlines methods for prevention including isolation of infected patients, hand hygiene, cleaning, sterilization, and disinfection to cut off routes of transmission and separate infection sources from the rest of the hospital.








































![INFECTION CONTROL[1] [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/infectioncontrol1read-only-231229080242-ead5802a-thumbnail.jpg?width=640&height=640&fit=bounds)





































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








