Downloaded 33 times
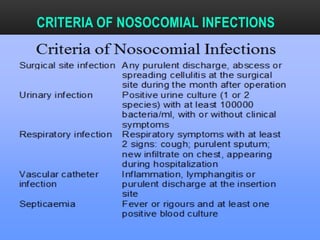
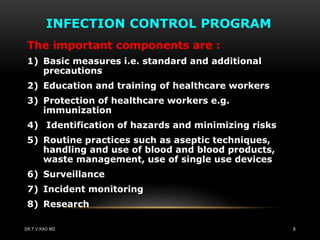
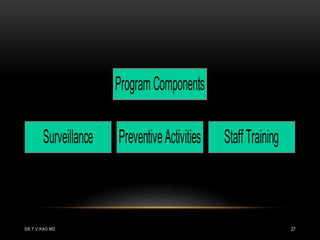
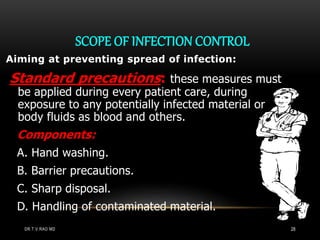




The document discusses the need for an infection control committee and outlines its proposed responsibilities. It describes different types of infections that can be acquired in a hospital setting. It also summarizes the key components of an infection control program, including surveillance, preventative activities, staff training, and an infection control manual. The roles of the infection control team and committee are defined in establishing standards and policies to minimize hospital-acquired infections.























































































