Downloaded 1,408 times
![Indications for induction of labor:
• Maternal indications
•
•
•
•
•
•
•
•
•
Post-term (main indication]
P.I.H (Timing depend )on the[ severity]
Diabetes Mellitus (increase risk
of baby loss and mortality rate)
Medical conditions (as renal, respiratory and
cardiac diseases)
Placenta insufficiency (as moderate or sever
placenta abruption but commonly C.S)
Prolonged pre-labor rupture of membranes.
Rheuses isoimmunization.
Maternal request.](https://image.slidesharecdn.com/inductionoflabor-140114033429-phpapp02/75/Induction-of-labor-4-2048.jpg)
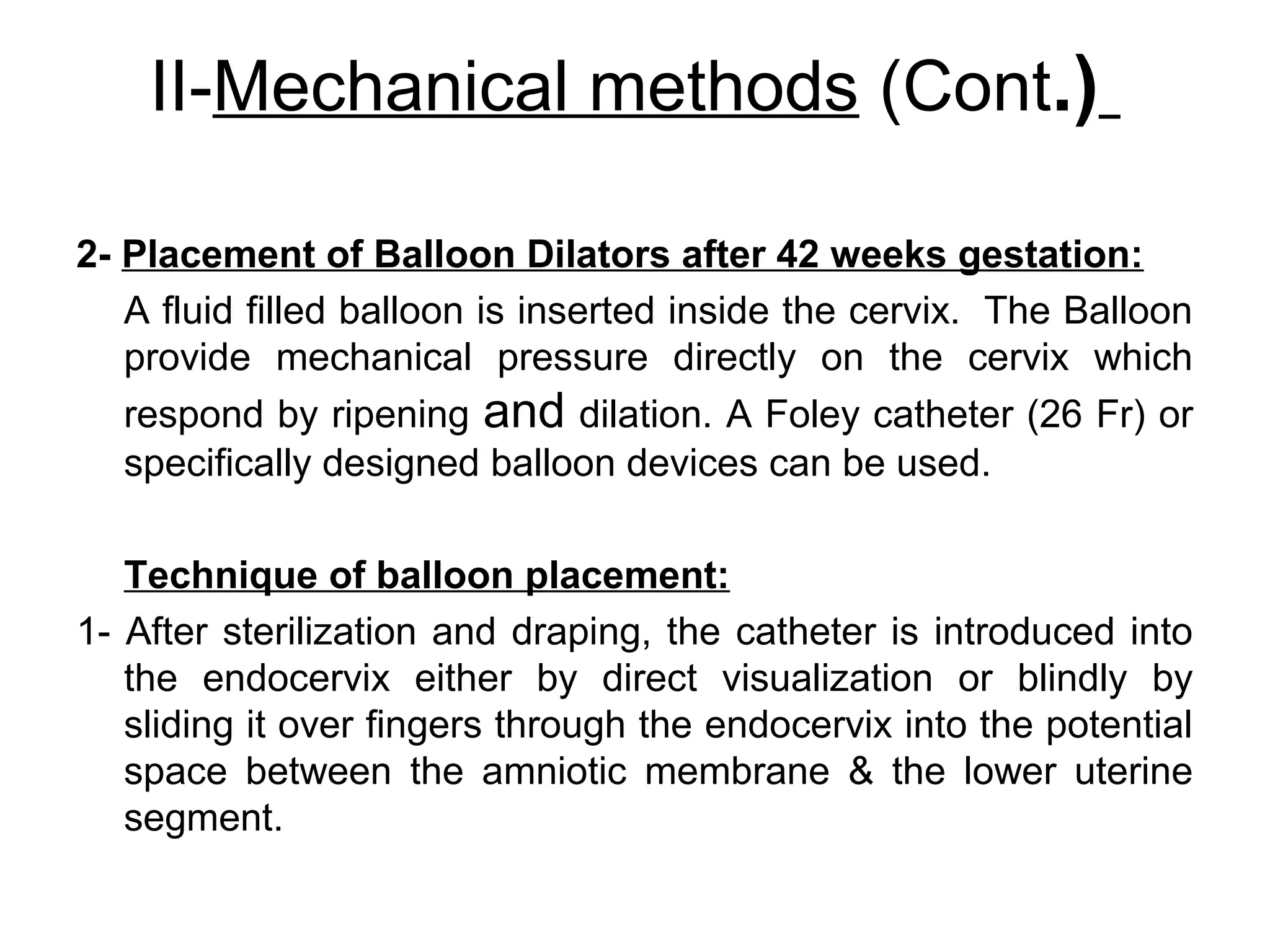
![III-Surgical Methods (Cont.)
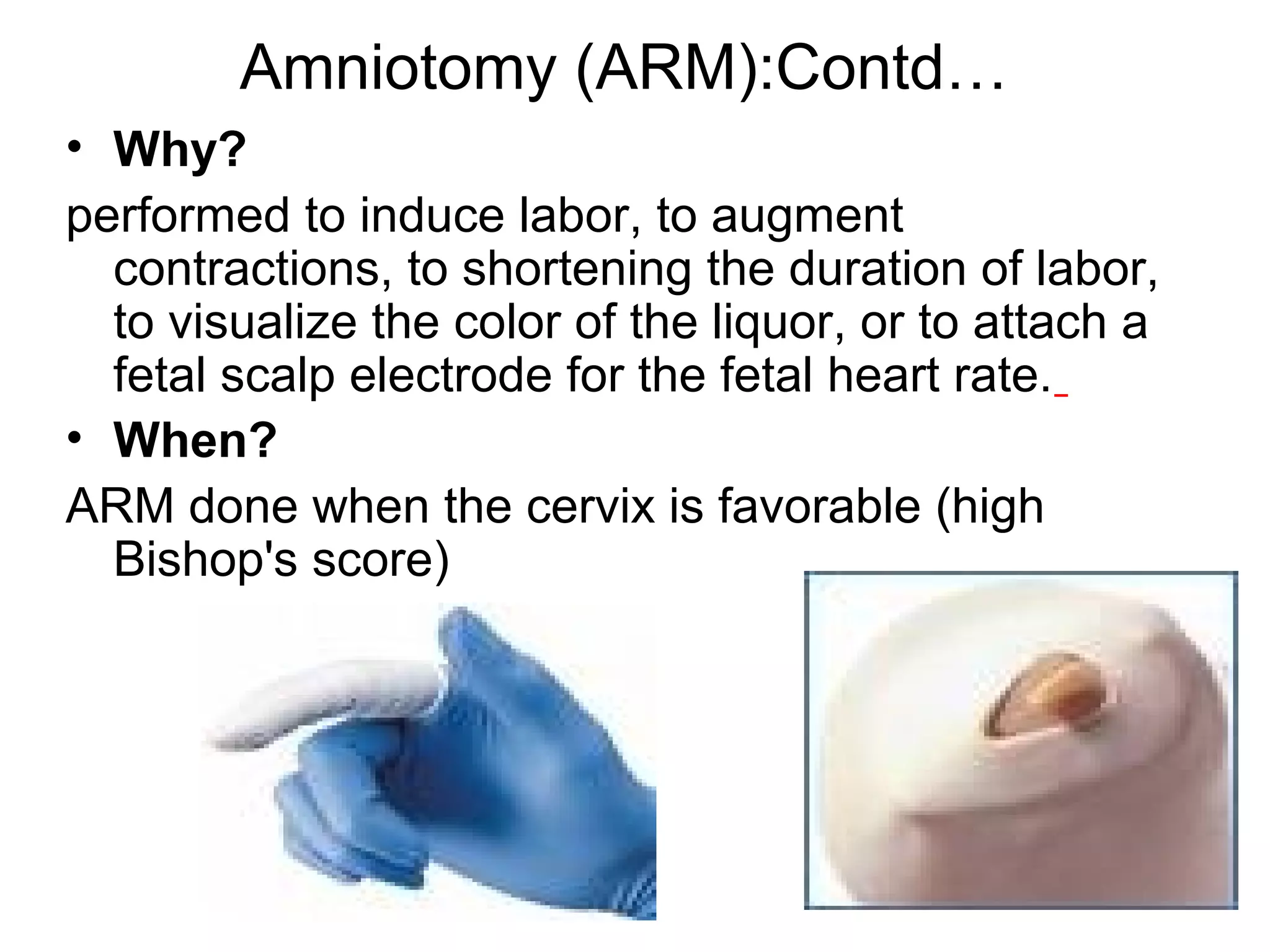
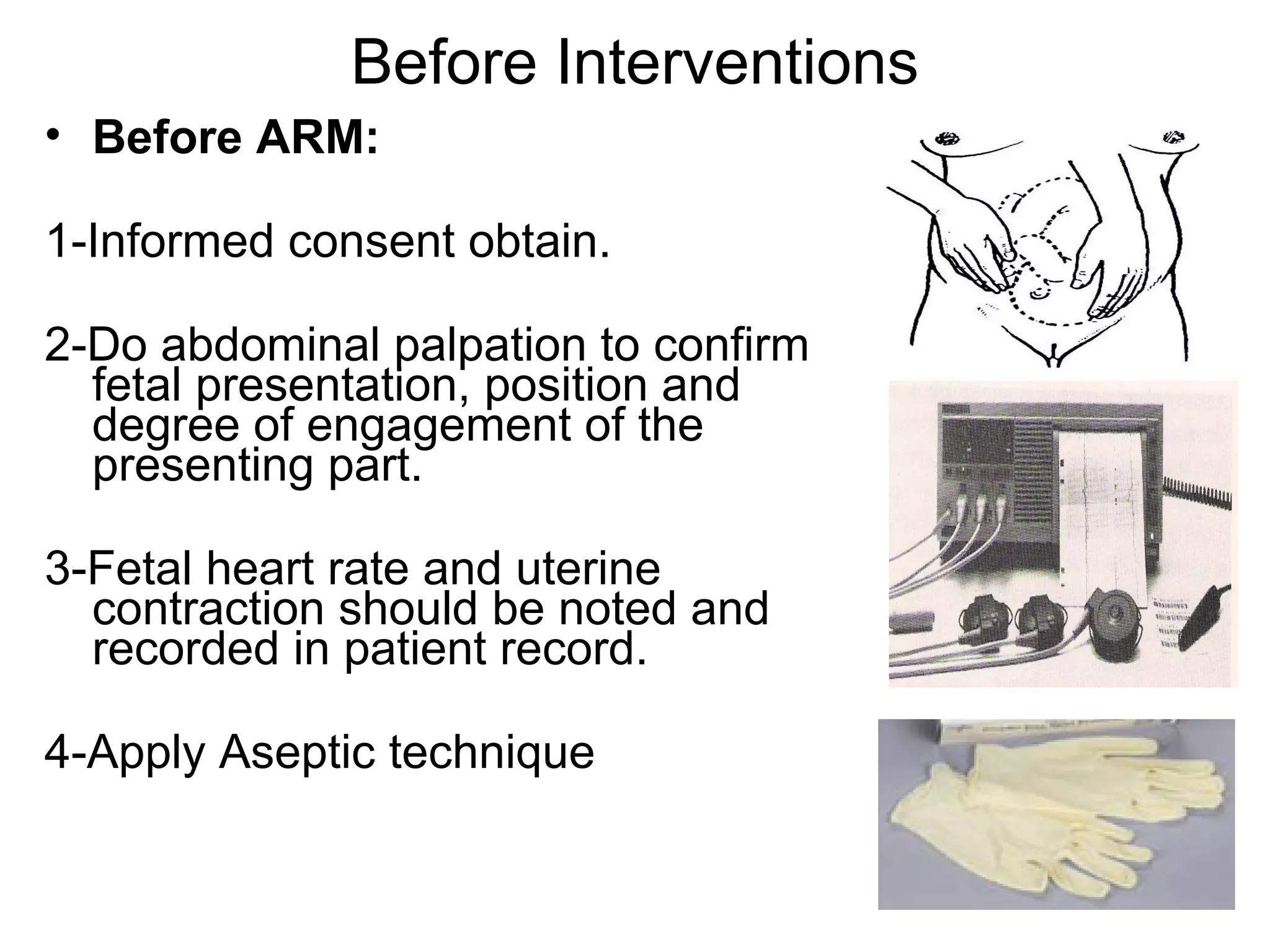
2-Amniotomy - Technique:
-The FHR is recorded before the procedure.
-A pelvic examination is performed to evaluate the cervix &
station of the presenting part. The presenting part should be
well fitted to the cervix.
-The membranes are identified and a kocher is inserted through
the cervical os by sliding it along the hand & fingers &
membranes are ruptured.
-Nature of the amniotic fluid is recorded
[clear,bloody,thick,thin,or meconium]
-The FHR is recorded after the procedure.](https://image.slidesharecdn.com/inductionoflabor-140114033429-phpapp02/75/Induction-of-labor-21-2048.jpg)








This document discusses induction of labor. It begins by defining induction of labor and listing its objectives. It then covers the indications and contraindications for induction, including maternal and fetal indications. It describes methods of induction, including natural non-medical methods, mechanical methods like hygroscopic dilators and balloon catheters, surgical methods like membrane stripping and amniotomy, and pharmacological methods using prostaglandins, misoprostol, mifepristone, and oxytocin. It provides details on techniques and risks of different methods. It emphasizes monitoring during inductions and lists side effects of pharmacological agents. The overall document is a guide for health professionals on selecting and performing appropriate induction methods for individual patients.























































































