Downloaded 914 times
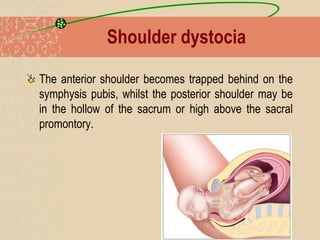
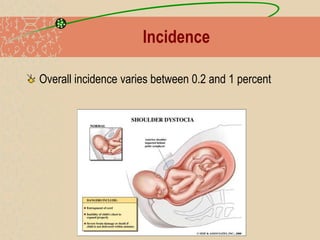

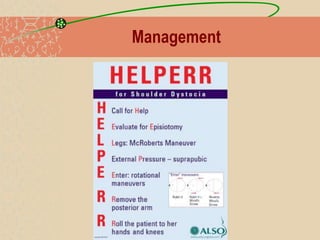
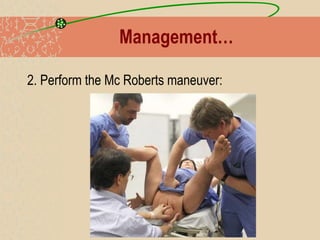
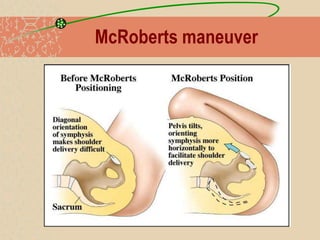
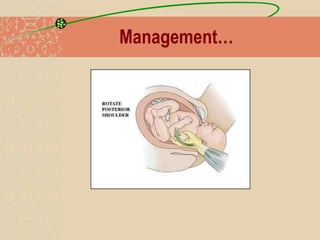
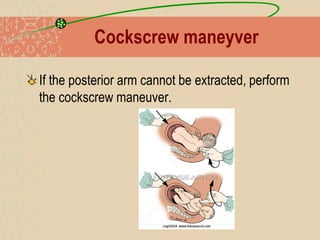

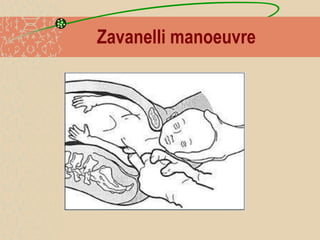

Shoulder dystocia occurs when the baby's shoulders become stuck after delivery of the head. It has a low incidence rate of 0.2-1% and risk factors include fetal macrosomia, obesity, diabetes and others. Diagnosis is made when normal maneuvers by the midwife fail to deliver the baby. Management involves calling for help, clearing the baby's airways, and performing maneuvers like McRoberts and Rubin's to rotate the shoulders and decrease their diameter in order to allow delivery. More invasive maneuvers like cleidotomy may be needed if these fail to deliver the anterior shoulder.