Downloaded 384 times


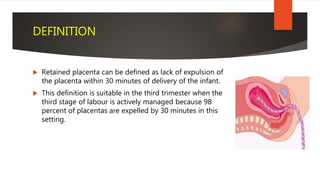









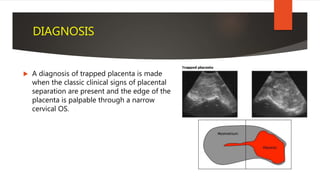




















The document discusses retained placenta, defined as the failure to expel the placenta within a specified time after delivery. It outlines various types of retained placenta, risk factors, and management strategies, emphasizing the importance of timely diagnosis and intervention due to possible complications such as postpartum hemorrhage. Effective management may involve techniques such as controlled cord traction, manual removal, and addressing underlying causes to facilitate placental expulsion.























































































