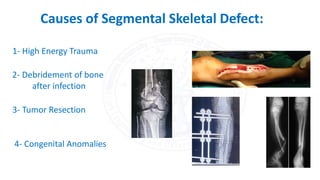







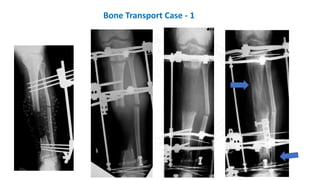
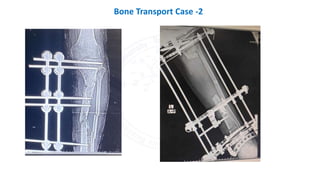
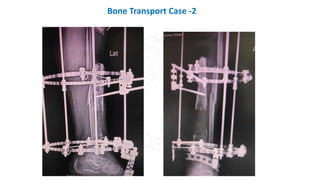
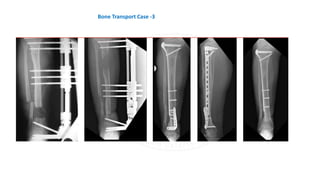


The document discusses the management of bone defects, particularly segmental defects that require intervention for healing. It outlines various causes, classifications, and treatment options, including autografts, vascularized grafts, membrane-induced techniques, and bone transport. Key factors influencing effective management include mechanical stability, a favorable biological environment, and considerations for patient health, such as tobacco cessation and glycemic control.
















































































