Downloaded 182 times

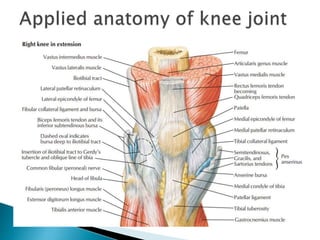

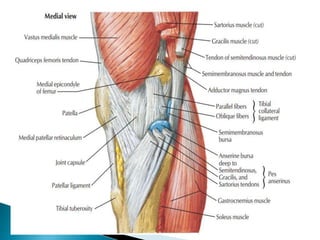
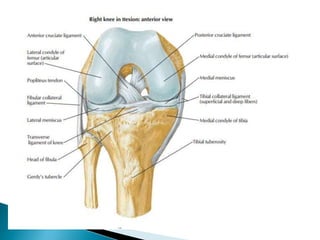
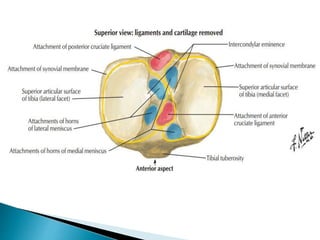
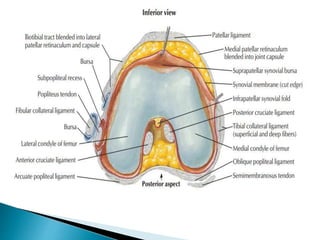
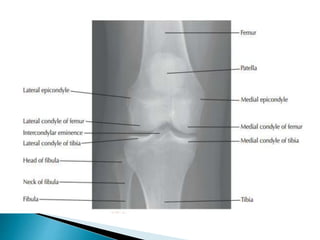

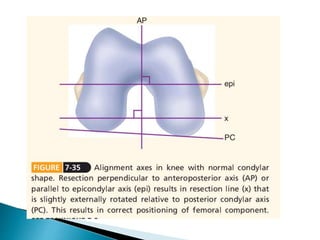


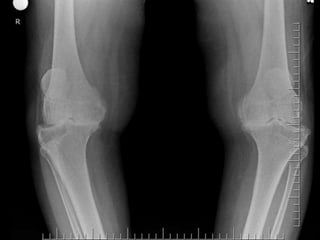

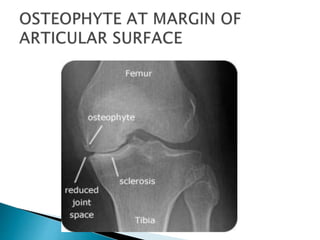
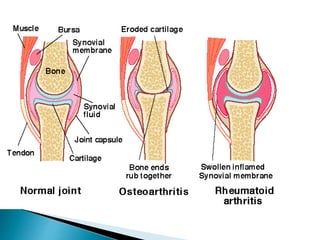

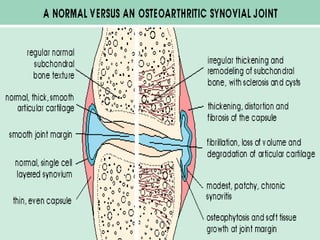


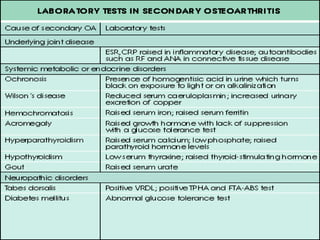

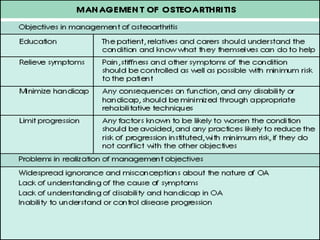





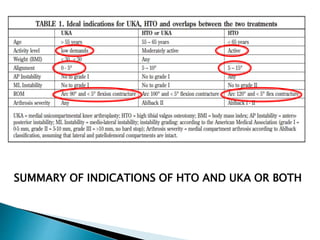
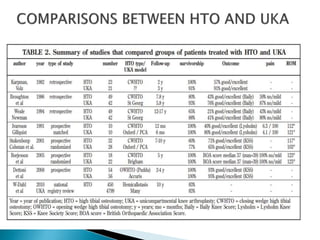


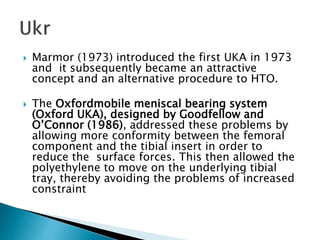

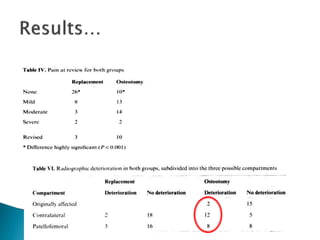
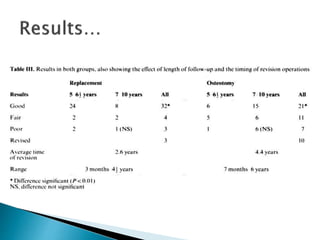



The document discusses osteoarthritis of the knee, including the anatomy and biomechanics of the knee joint, risk factors and clinical features of osteoarthritis, conservative and surgical management options. Specifically, it focuses on unicondylar knee arthroplasty versus high tibial osteotomy for the treatment of unicondylar osteoarthritis of the knee, outlining the indications, types of implants, and contraindications for unicondylar knee arthroplasty.





























































































