2. DEFINITION
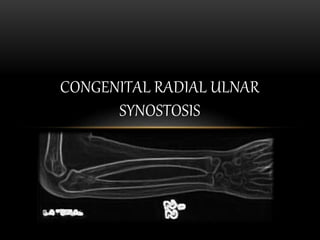
• Congenital Radial Ulnar
Synostosis is a congenital
condition caused by failure
of differentiation that leads
to the presence of a bony
bridge between the
proximal radius and ulna.
3. ETIOLOGY
• Pathophysiology
• Forearm begins as a single cartilaginous unit
and divides from distal to proximal into the radius
and ulna in the 7th week in utero
• Failure of differentiation results in synostosis
in proximal aspect of the forearm.
4. ETIOLOGY
• Genetics
• Familial cases with autosomal dominant
inheritance
• Associated with chromosomal abnormalities,
particularly duplication of sex chromosomes
• 20% with positive family history
5. ETIOLOGY
• Associated syndromes (30%)
• Apert syndrome (acrocephalosyndactyly)
• Carpenter's syndrome
(acropolysyndactlyly)
• Arthrogryposis
• Mandibulofacial dysostosis
• Klinefelter's syndrome (XXY) and other sex
chromosome abnormalities
6. PRESENTATION
• SYMPTOMS
• Painless
• Most commonly asymptomatic, noticed by parents and teachers
• Difficulty with specific tasks
• Keyboard, tabletop activities - deficient pronation
• Eating, washing face, catching a ball - deficit supination
7. PRESENTATION
• PHYSICAL EXAMINATION
• Average age of diagnosis is 6 years of
age
• Can go unnoticed until early
adolescence, especially in
unilateral cases
• Elbow flexion usually preserved
• Fixed forearm pronation
• Average position is 30° of pronation
8. PRESENTATION
• Compensatory motion
• Shoulder abduction -
compensates for loss
of active pronation
• Shoulder adduction -
compensates for loss
of active supination
• Wrist hypermobility
9. IMAGING
• Radiographs recommended views
• AP and Lateral of forearm and
elbow
• Findings
• Can see proximal synostosis
• Radius is wide and bowed
• Ulna is narrow and straight
• Radial head may be dislocated
and/or malformed
14. TREATMENT
• Operative
• Indications
• Absolute
• Deformity is limiting
ability to participate in
specific activities
(sports, hygiene, eating)
• Relative
• Severe pronation
deformity > 60°
• Bilateral deformities
15. TREATMENT
• Operative
• General options
• Mobilization of the synostosis - to restore
active forearm rotation
• Rotational osteotomy - to improve static
forearm and hand position
16. TREATMENT
• OPERATIVE
SYNOSTOSIS EXCISION WITH SOFT TISSUE
INTERPOSITION
Goal: Restore active forearm rotation
• Technique
• Excise synostosis and interpose vascularized
fascio-fat graft
• Vascularized fat better than free fat graft
• Interposed anconeus muscle did not
prevent reossification
• Excision alone without graft interposition
results in nearly 100% recurrence of
synostosis
17. TREATMENT
• OPERATIVE
SYNOSTOSIS EXCISION WITH SOFT TISSUE
INTERPOSITION
Outcomes
• Gain in active forearm motion is usually
slight
• Unsatisfactory results in most studies
18. TREATMENT
• Operative
• FOREARM DEROTATIONAL
OSTEOTOMY
• Goal
• Place the forearm in more
functional resting position
• Technique
• Perform between 3-6 years of
age (average age ~5 years)
•
19. TREATMENT
• Operative
• Forearm Derotational osteotomy
• Osteotomy location
• Radius and ulna diaphysis
distal to synostosis, at
different levels
• Osteotomies at different
levels distributes
rotational correction - less
soft tissue tightness and
risk of neurovascular
complications
20. TREATMENT
• Operative
• Forearm Derotational osteotomy
• Osteotomy location
• Radius and ulna proximal
diaphysis at synostosis
• Rotation takes place over
narrow space - risks soft
tissue tightness, loss of
correction and
neurovascular
compromise
21. TREATMENT
• Operative
• Forearm Derotational osteotomy
Radius distal diaphysis alone
• Timing of correction
• Immediate correction - at time of
osteotomy
• Delayed correction - 10 days
following osteotomy
• Gradual correction with circular
external fixator frame (ilizarov)
22. TREATMENT
• Lowest rate of neurovascular complications (compartment
syndrome, nerve palsies) seen in Gradual correction with
circular external fixator frame (ilizarov)
• Positioning
• Unilateral - fix the forearm in 0-30° pronation
• Bilateral - fix dominant forearm in 0-15°
pronation and nondominant forearm in neutral
23. TREATMENT
• Operative
• Stabilization
• Casting alone (no fixation)
• Circular external fixator frame (ilizarov)
• Percutaneous pins
• Outcomes
• Most techniques result in improved forearm position and
patient function with low rate of deformity recurrence
24. COMPLICATION
• Recurrence of synostosis
• Nearly 100% recurrence of synostosis with excision alone or
with interposition of anconeus muscle
• Interposition of vascularized fascio-fat graft has 0%
recurrence
• Recurrence of malrotation
• Casting after derotational osteotomy associated with 15-20°
loss of correction
25. COMPLICATION
• Compartment syndrome
• Up to 36%
• Associated with large rotational
corrections > 60°
• Close observation post-operatively
• Some authors advocate for
prophylactic forearm fasciotomies
in acute and/or large deformity
corrections
26. COMPLICATION
• Neurologic deficit
• PIN palsy - particularly with
proximal (synostosis)
osteotomy
• AIN palsy
• Radial nerve palsy
• Higher risk with acute/large
deformity correction
• Most resolve within 3 months