Downloaded 133 times





![IVU (contrast urography= intravenous pyelography [IVP]= excretory urography) Pelvi-abdominal CT is sensitive for diagnosing obstructive nephropathy and is used when obstruction cannot be shown by ultrasonography or by intravenous urography. © By Mohammed Ibrahim, MBBcH Revised by M.A.Wadood , MD, MRCS DIAGNOSIS By Moh.Ibrahim, MBBcH Revised by M.A.Wadood , MD, MRCS](https://image.slidesharecdn.com/bphandobstructiveuropathy2-120206155508-phpapp01/85/BPH-and-Obstructive-Uropathy-8-320.jpg)



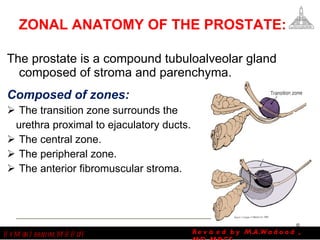
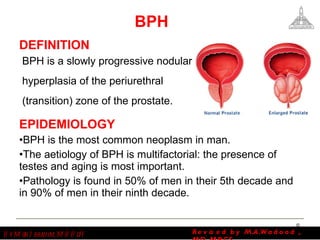




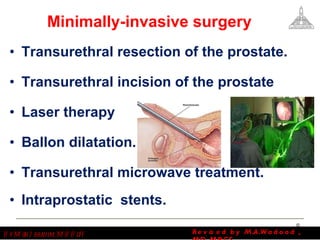
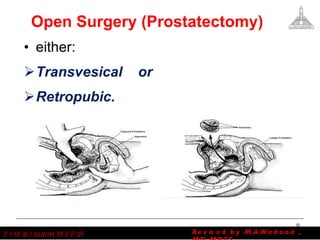


The document discusses obstructive uropathy and benign prostatic hyperplasia (BPH). It defines obstructive uropathy as structural or functional hindrance of normal urine flow. BPH is defined as a slowly progressive nodular hyperplasia of the periurethral zone of the prostate. The document outlines causes, symptoms, diagnostic tests and treatments for both conditions. Treatments include medications, minimally invasive surgeries such as transurethral resection of the prostate, and open surgeries like prostatectomy.









































































