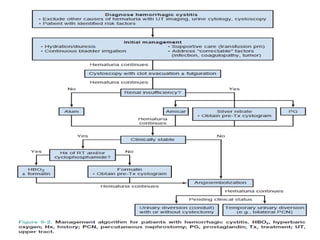
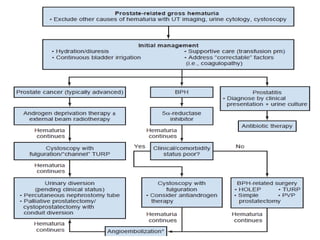
The document discusses various treatment options for managing hematuria, including intravesical alum irrigation, formalin, hydrostatic pressure, embolization, hyperbaric oxygen therapy, and sodium pentosanpolysulphate. Each method is detailed with protocols, side effects, and success rates, emphasizing the importance of specific preparations and monitoring during procedures. Overall, the document provides a comprehensive overview of the strategies for addressing intractable hematuria in clinical practice.








































![BLADDER_IRRIGATION[1] Mr. Tarique. 23.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bladderirrigation1tarique-240529154658-6896ec03-thumbnail.jpg?width=640&height=640&fit=bounds)






























![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)


