Downloaded 367 times




















![Usual interstitial pneumonia
Usual interstitial pneumonia (UIP) is a form of lung disease characterized
by progressive scarring of both lungs.[1]
The scarring (fibrosis) involves the supporting
framework (interstitium) of the lung. UIP is thus classified as a form of
interstitial lung disease. The term "usual" refers to the fact that UIP is the most common
form of interstitial fibrosis. "Pneumonia" indicates "lung abnormality", which includes
fibrosis and inflammation. A term previously used for UIP in the British literature is
cryptogenic fibrosing alveolitis, a term that has fallen out of favor since the basic
underlying pathology is now thought to be fibrosis, not inflammation.
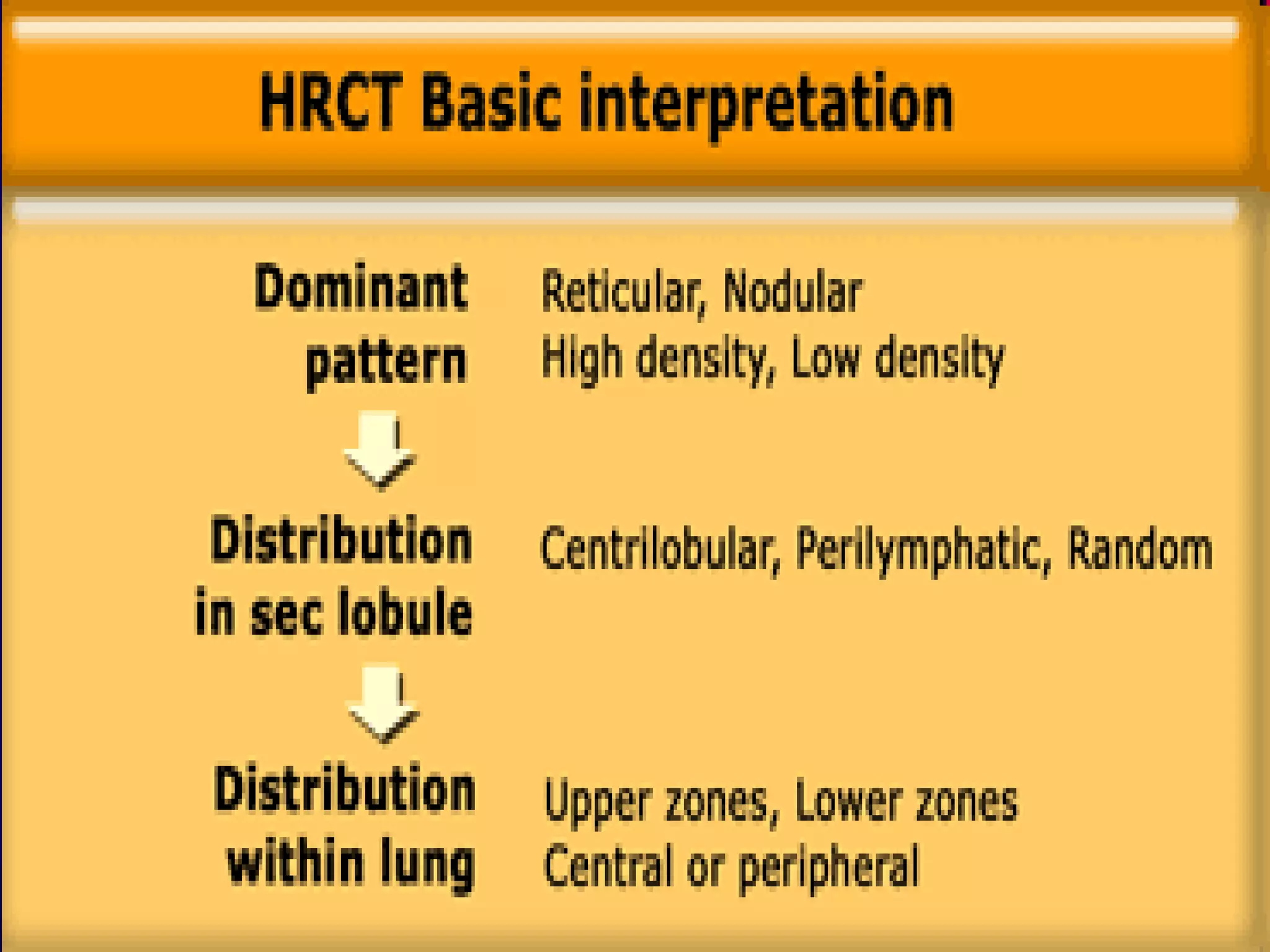
Location: distribution
The distribution of UIP on CT images is typically characteristically with an
apico-basal gradient with basal and peripheral predominance, although it is
often patchy.
Typical features include 1,5
:
the presence of reticular opacities in the immediate subpleural lung,
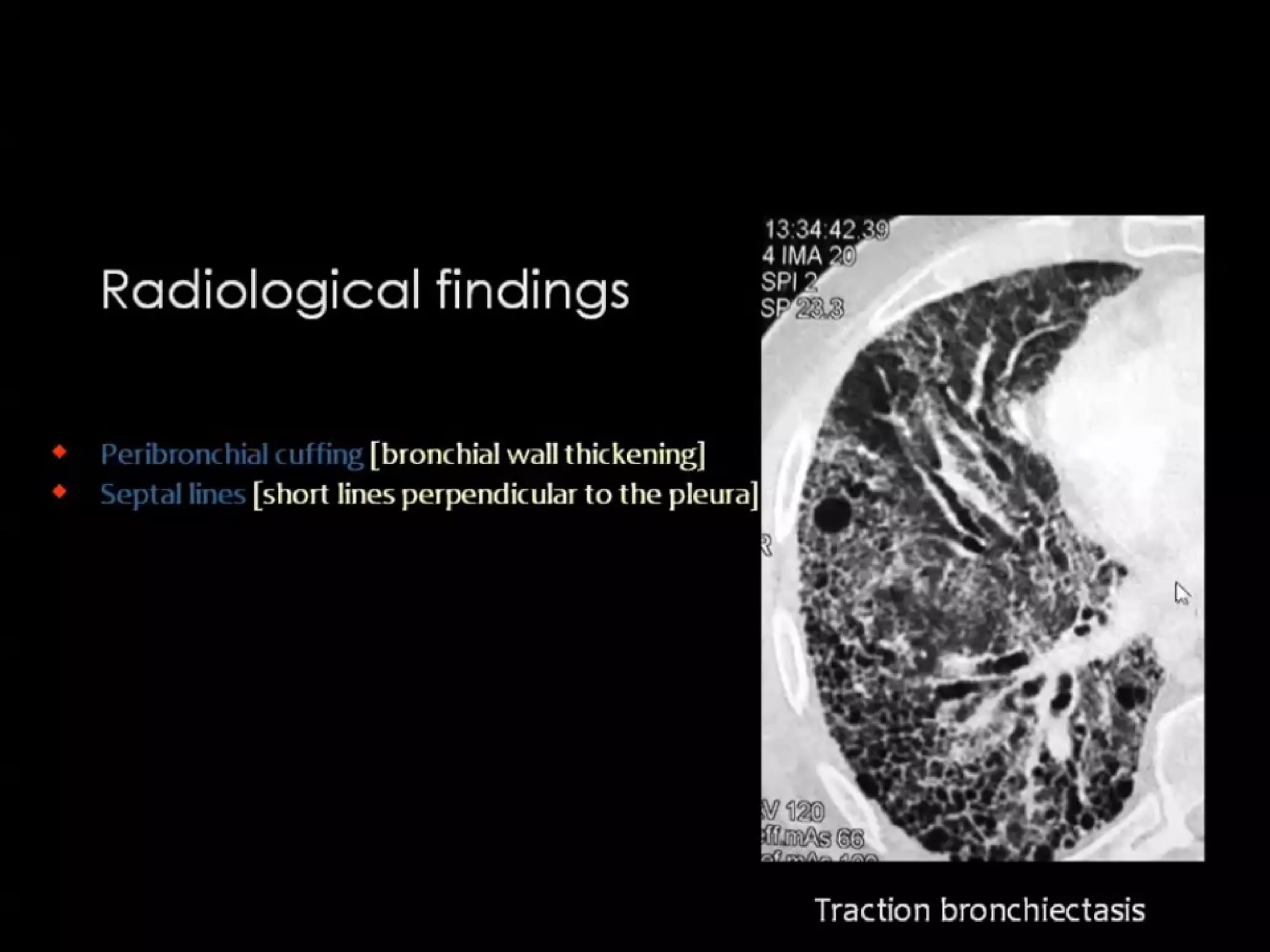
often associated with honeycombing and/ or traction bronchiectasis,](https://image.slidesharecdn.com/hrct-1-151125084839-lva1-app6891/75/HRCT-Reticular-pattern-39-2048.jpg)



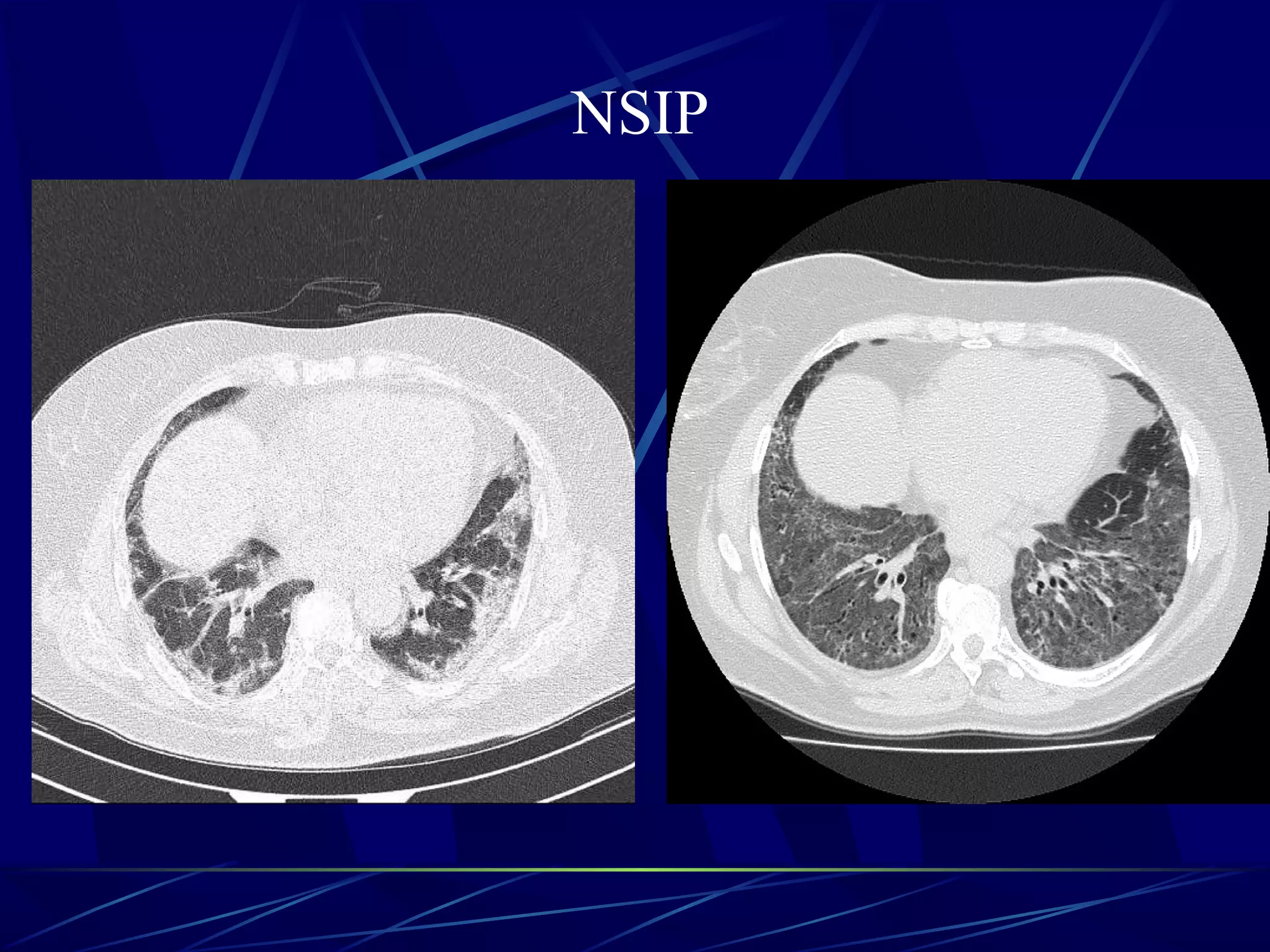














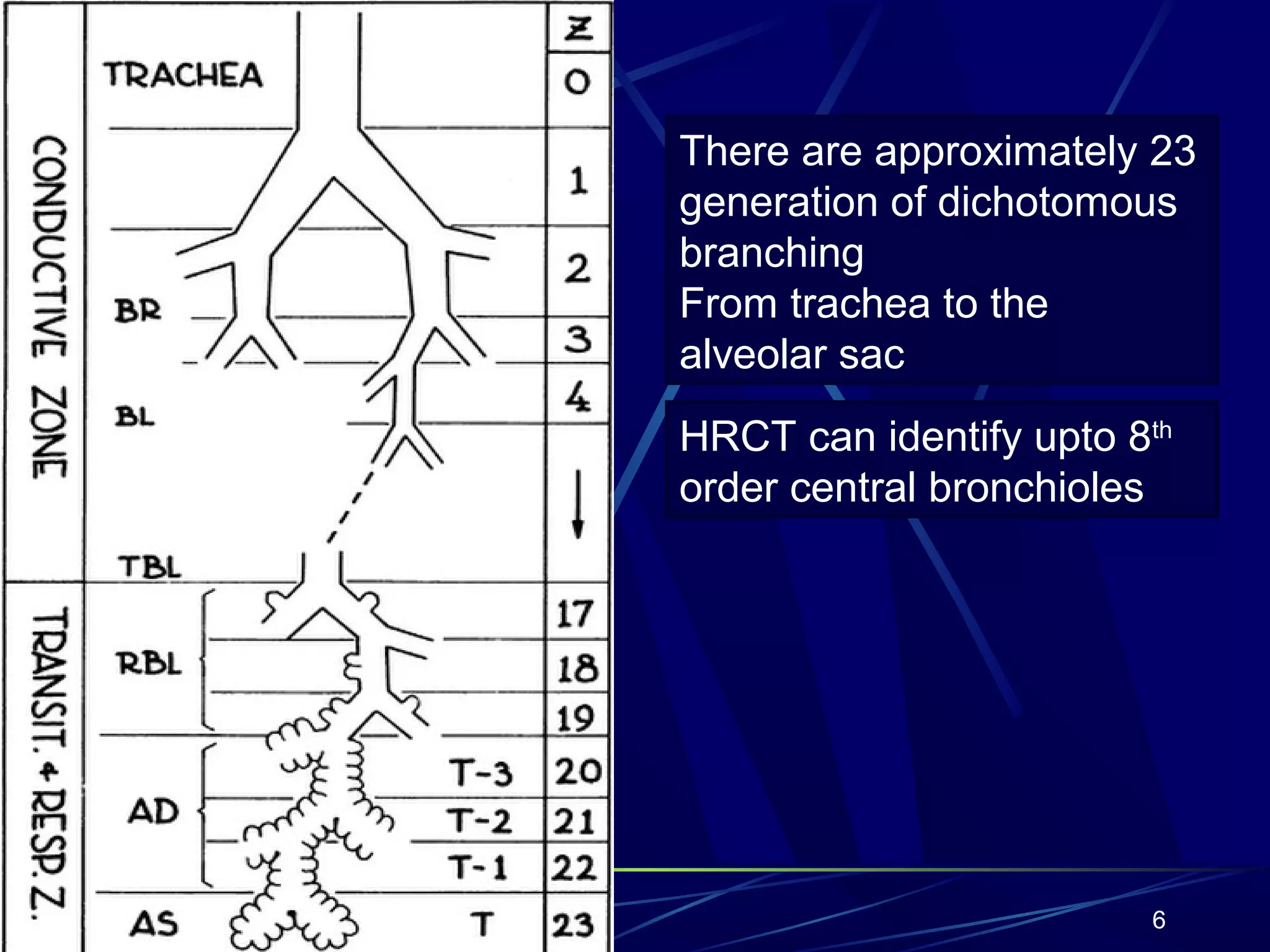
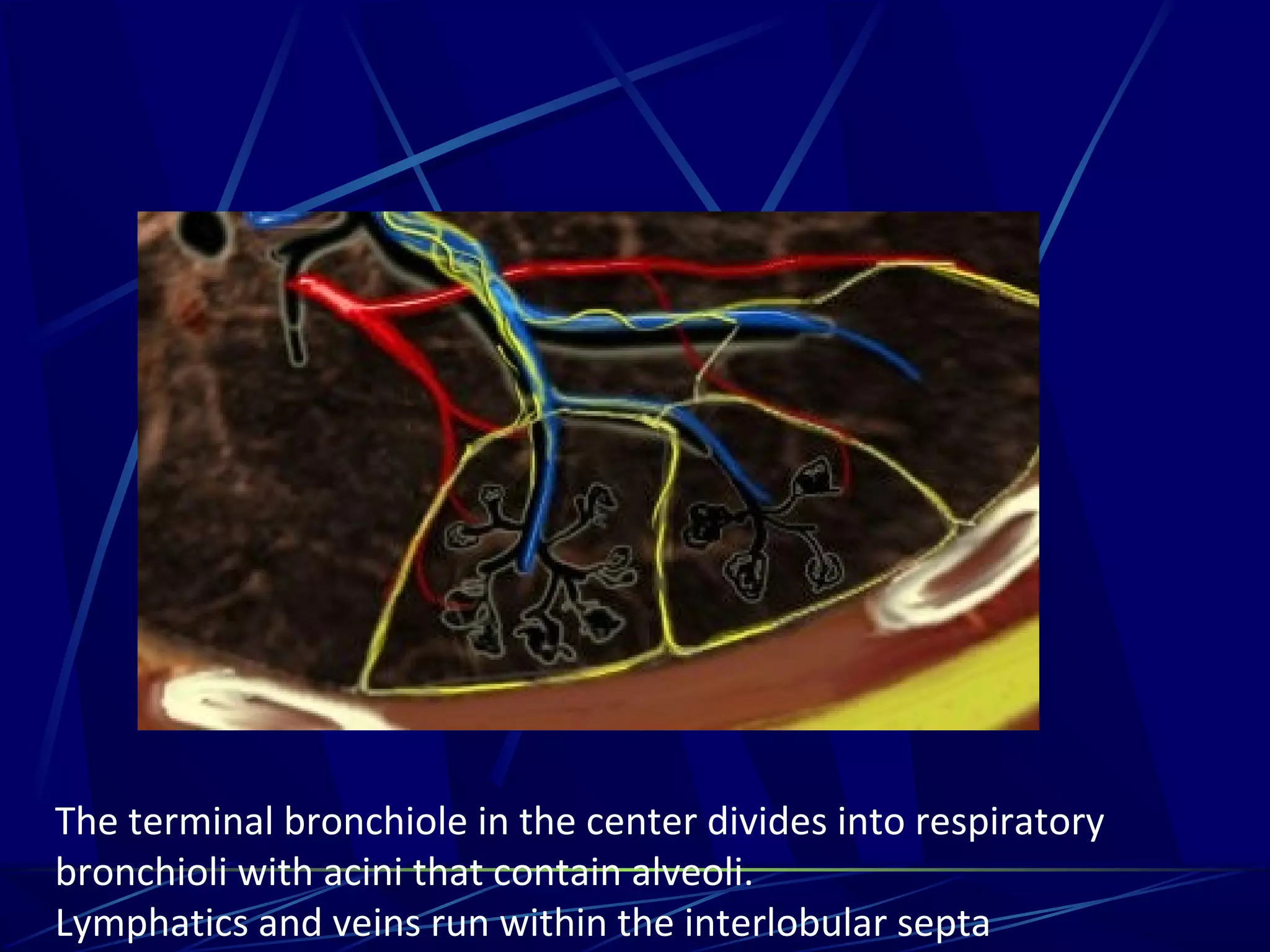
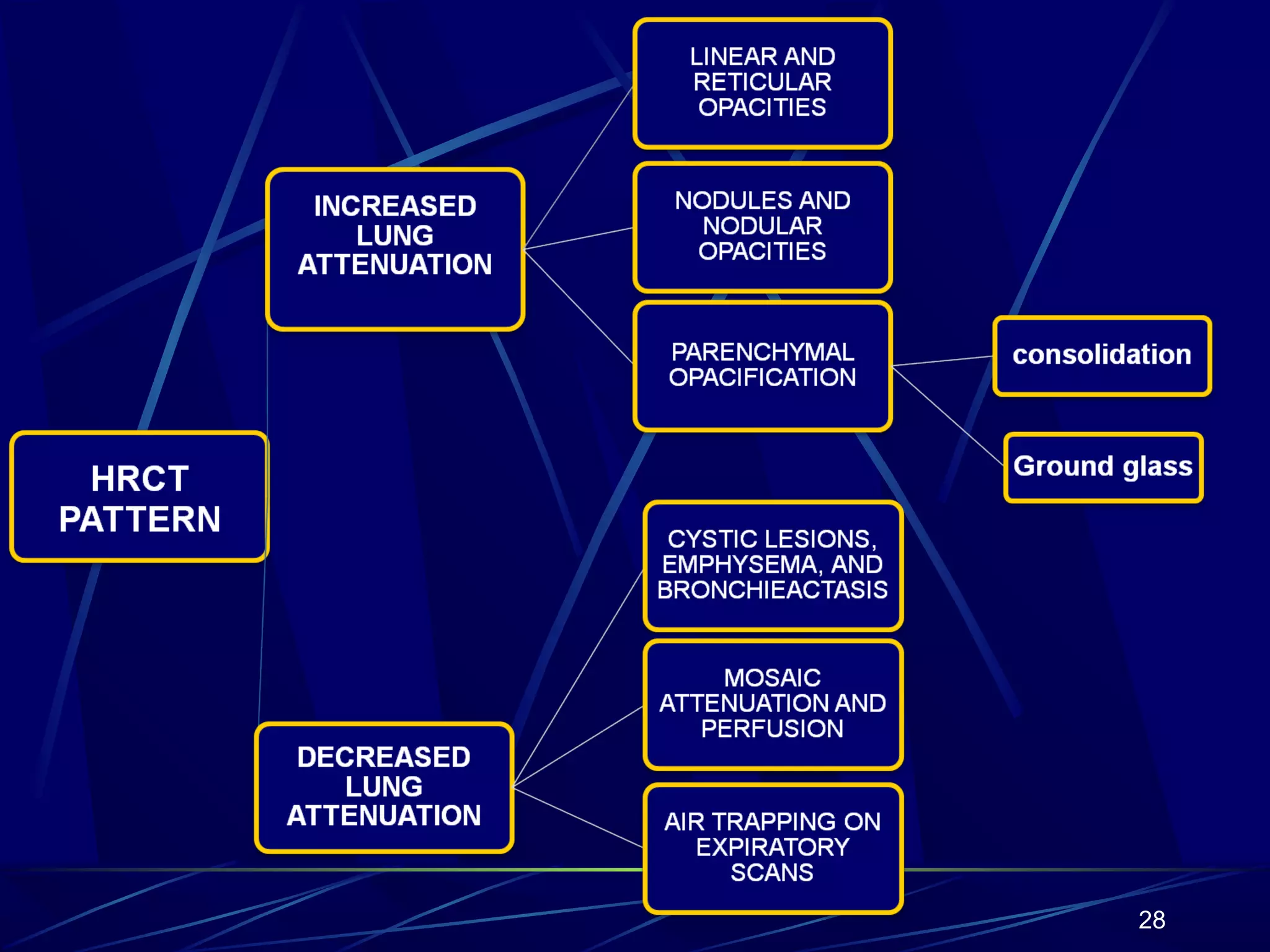
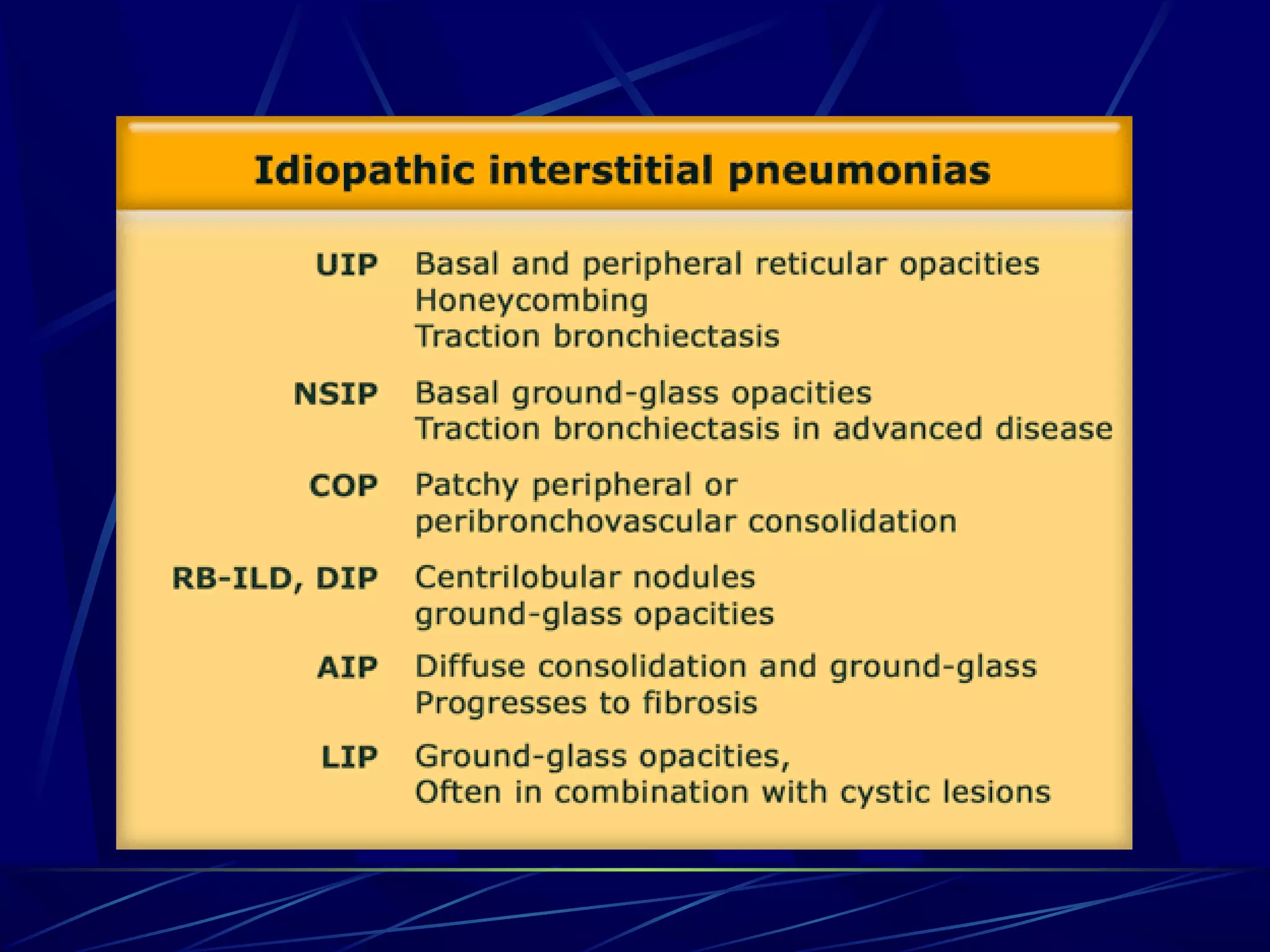
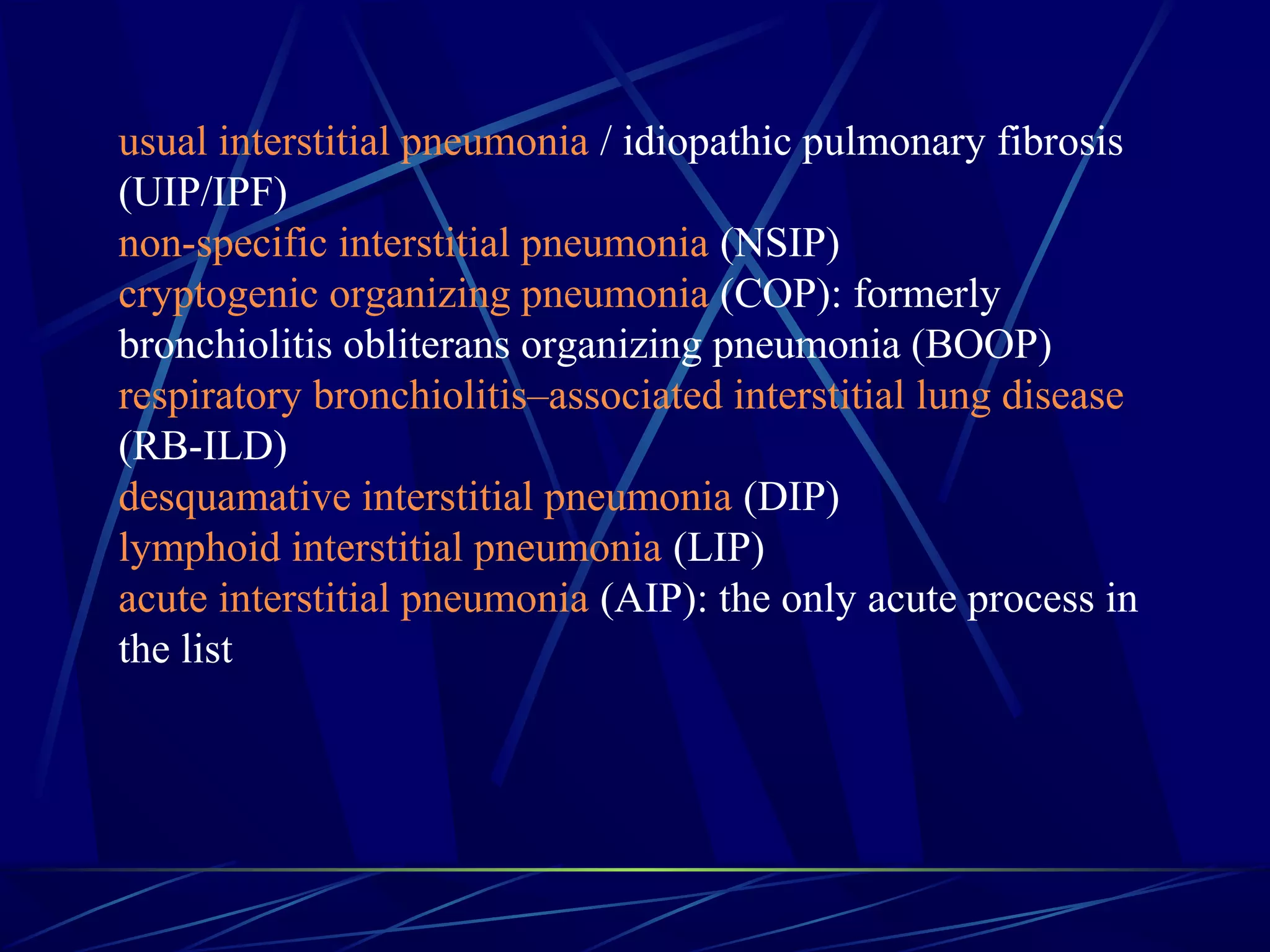
The document provides a detailed overview of High-Resolution Computed Tomography (HRCT) in diagnosing pulmonary diseases, emphasizing its superiority over traditional chest radiography. It discusses the anatomy of the secondary lobule, various patterns of interstitial lung diseases, and specific conditions like Usual Interstitial Pneumonia (UIP) and Non-Specific Interstitial Pneumonia (NSIP). Additionally, it outlines differential diagnoses and the impact of factors such as drug toxicity and radiation on lung health.








































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










