• Basic anatomicunit
• Smallest lung unit surrounded by connective tissue
septa
• Measures 1-2 cm
• Made up of 5-15 pulmonary acini, that contain the
alveoli
• Supplied by a small bronchiole (terminal bronchiole)
in the center, that is parallelled by the centrilobular
artery
• Pulmonary veins and lymphatics run in the periphery
of the lobule within the interlobular septa
• Two lymphatic systems: central network-
bronchovascular bundle towards the centre of the
lobule ; peripheral network- within the interlobular
septa and along the pleural linings
7.
What is thedominant HR-pattern:
❖ Reticular
❖ Nodular
❖ High attenuation (ground-glass, consolidation)
❖ Low attenuation (emphysema, cystic)
Where is it located within the secondary lobule (centrilobular,
perilymphatic or random)
Is there an upper versus lower zone or a central versus
peripheral predominance
Are there additional findings (pleural fluid, lymphadenopathy,
traction bronchiectasis)
BASIC
INTERPRETATION
9.
RETICULAR PATTERN
Thickening ofthe interlobular septa / fibrosis as in
honeycombing
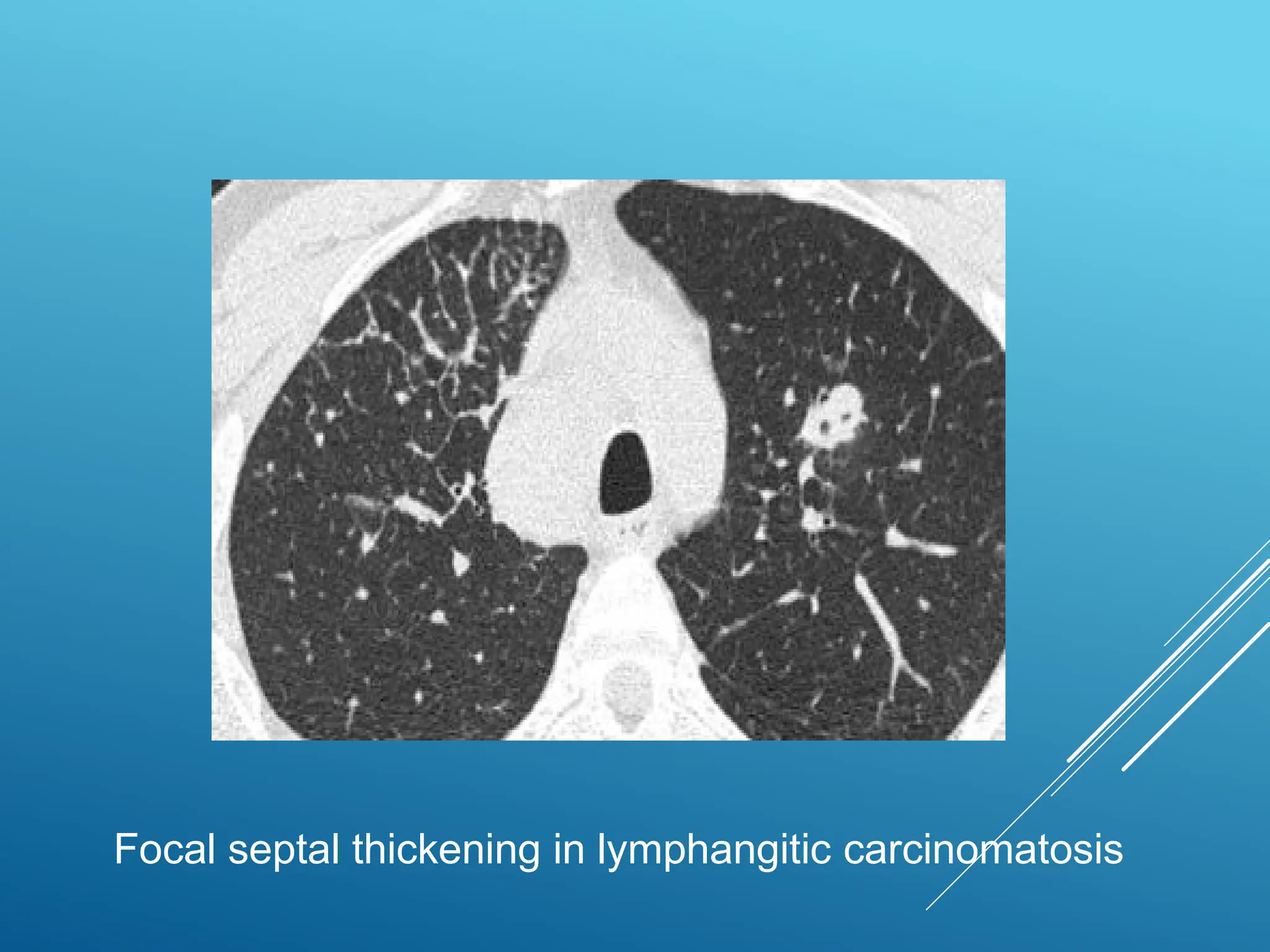
SEPTAL THICKENING
Thickening of lung interstitium by fluid, fibrous tissue, or
infiltration by cells results in a pattern of reticular
opacities due to thickening of the interlobular septa
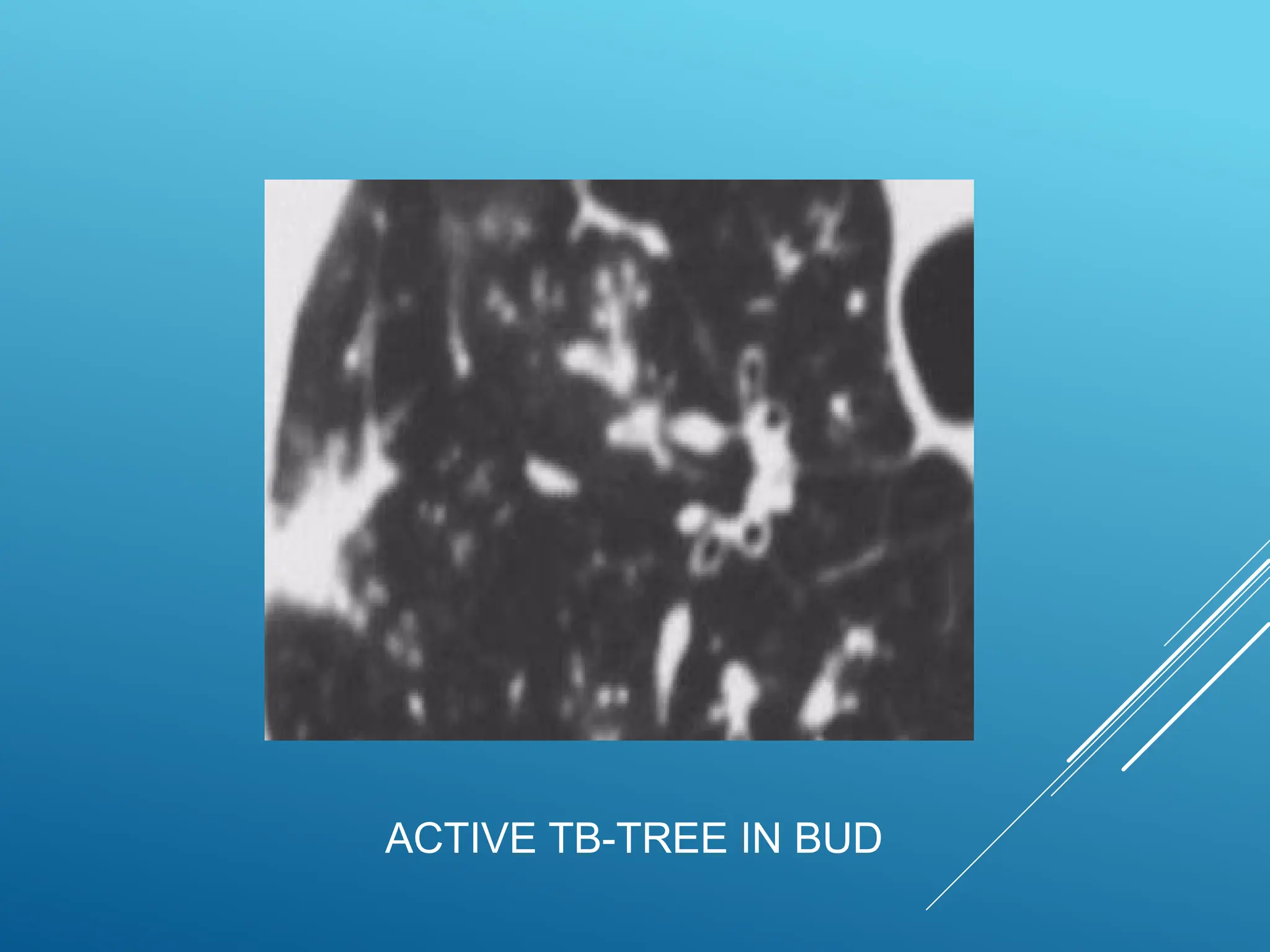
✓ TREE-IN-BUD APPEARANCE:
✓Irregular and nodular branching structure, most easily identified in
the lung periphery
✓ Represents dilated and impacted (mucus or pus-filled) centrilobular
bronchioles
17.
Tree-in-bud indicates thepresence of:
Endobronchial spread of infection (TB, MAC, any
bacterial bronchopneumonia)
Airway disease associated with infection (cystic fibrosis,
bronchiectasis)
Airway disease associated primarily with mucus retention
(allergic bronchopulmonary aspergillosis, asthma)
RANDOM NODULES
Resultof the hematogenous spread of the infection
Small random nodules are seen in:
• Haematogenous metastases
Miliary tuberculosis
Sarcoidosis may mimick this pattern, when very
extensive.
Langerhans cell histiocytosis (early nodular stage)
21.
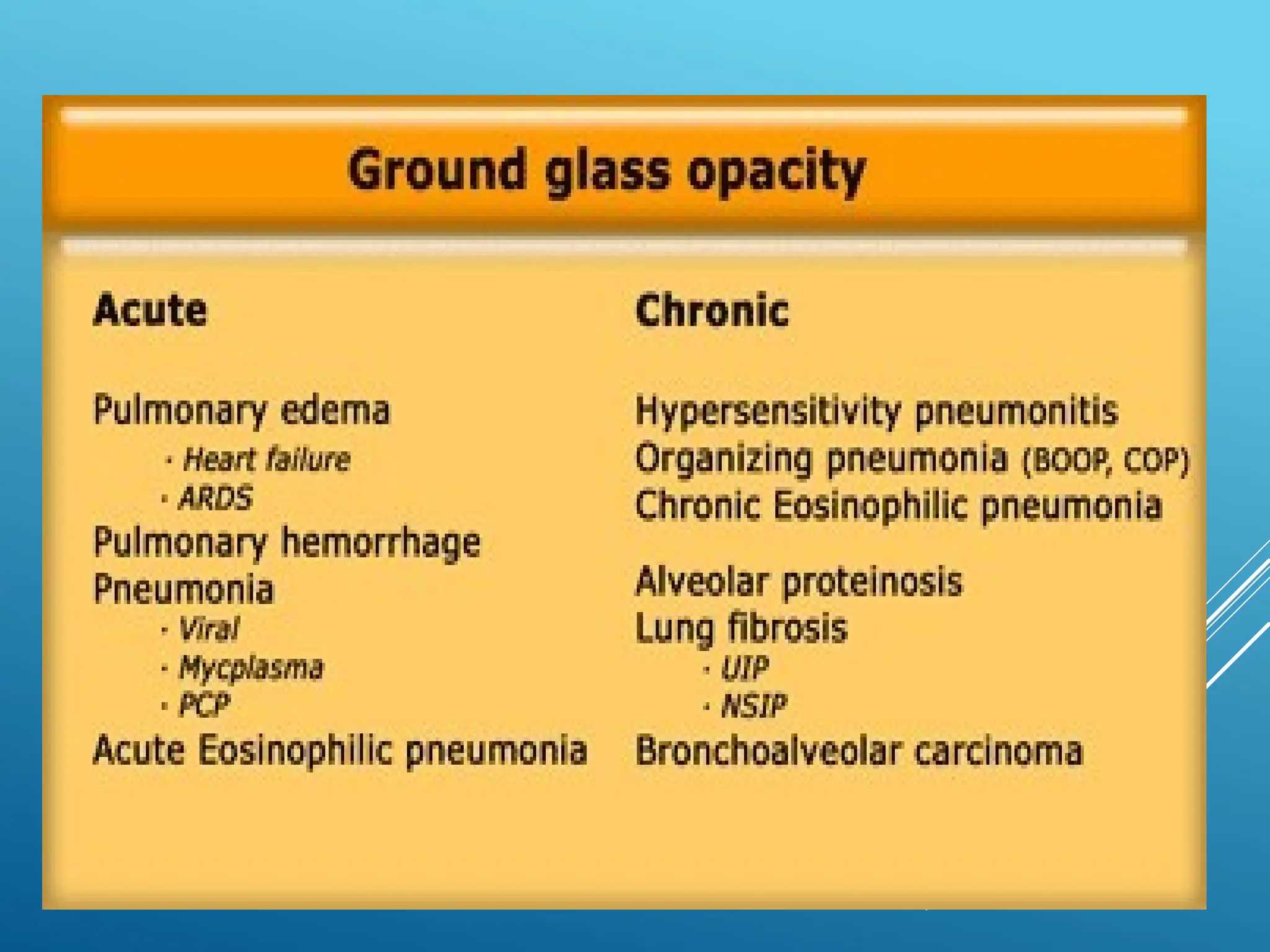
✓ Ground-glass-opacity =hazy increase in lung opacity
without obscuration of underlying vessels
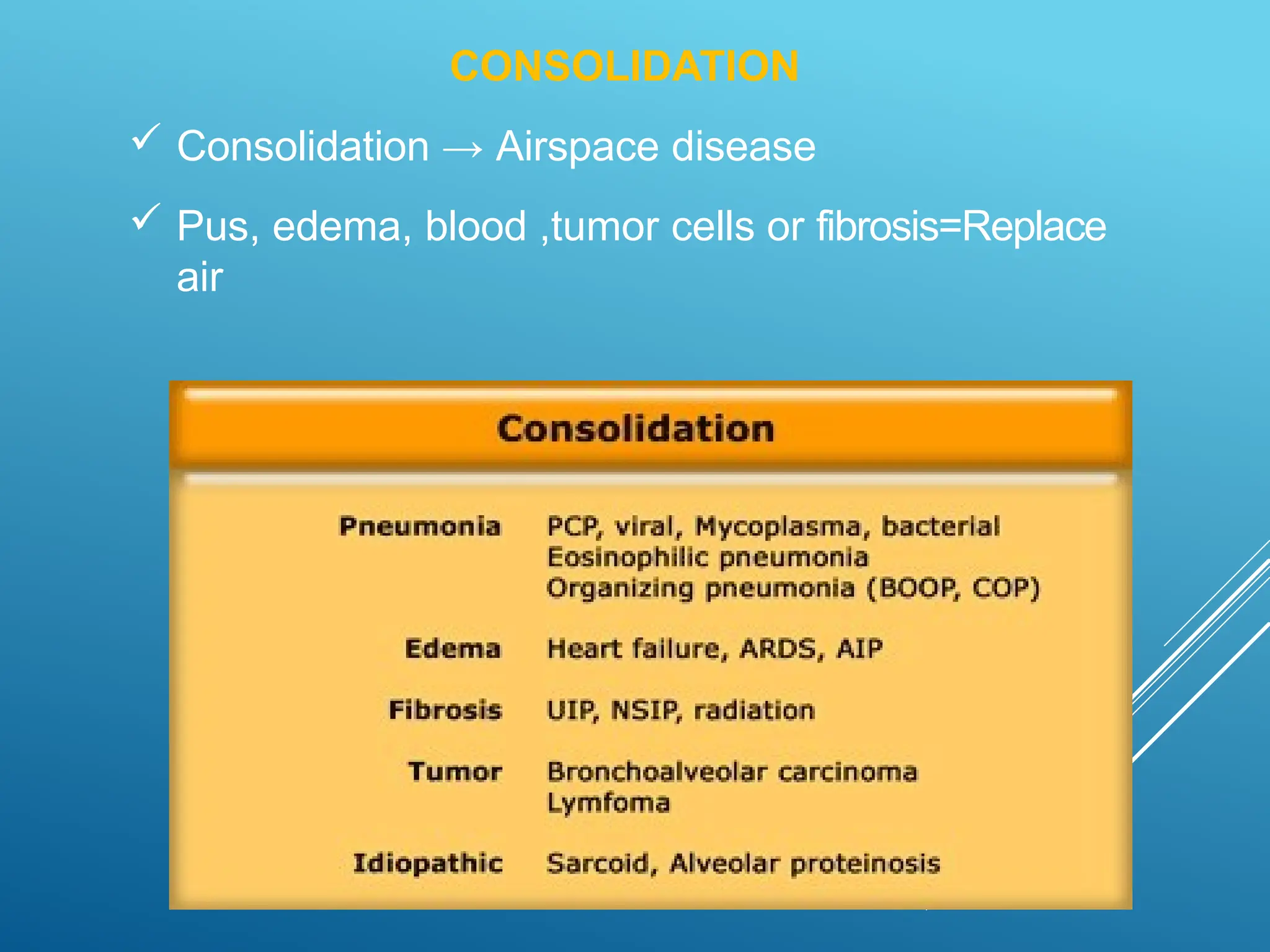
✓ Consolidation = increase in lung opacity which
obscures the vessels
HIGH ATTENUATION PATTERN
22.
GROUND-GLASS OPACITY →FILLINGOF THE
ALVEOLAR SPACES WITH PUS, EDEMA,
HEMORRHAGE, INFLAMMATION OR TUMOR
CELLS→THICKENING OF THE INTERSTITIUM OR
ALVEOLAR WALLS BELOW THE SPATIAL
RESOLUTION OF THE HRCT AS SEEN IN FIBROSIS
✓ Upper zone predominance: Respiratory bronchiolitis,
PCP
✓ Lower zone predominance: UIP, NSIP, DIP
✓ Centrilobular distribution: Hypersensitivity pneumonitis,
Respiratory bronchiolitis
24.
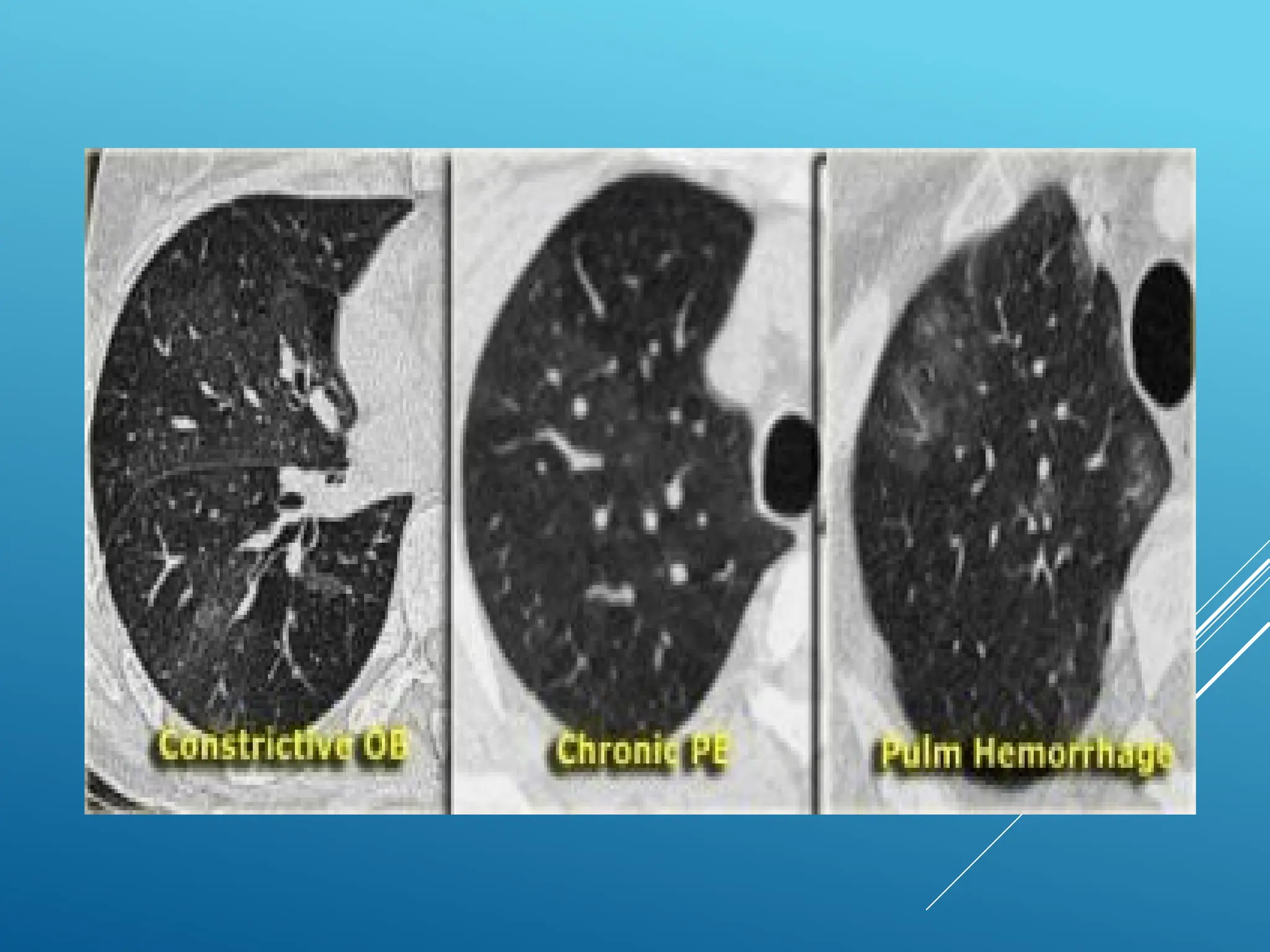
'Mosaic attenuation' =density differences between affected
and non-affected lung areas
When ground glass opacity presents as mosaic attenuation
to consider:
Infiltrative process adjacent to normal lung
Normal lung appearing relatively dense adjacent to
lung with air-trapping
Hyperperfused lung adjacent to oligemic lung due
to chronic thromboembolic disease
MOSAIC ATTENUATION
LOW ATTENUATION PATTERN
Decreasedlung attenuation or air-filled lesions.
These include:
Emphysema
Lung cysts (LAM, LIP, Langerhans cell
histiocytosis)
Bronchiectasis
Honeycombing
32.
Areas of lowattenuation without visible walls as a result of
parenchymal destruction
Centrilobular emphysema
✓ Most common type
✓ Irreversible destruction of alveolar walls in the
centrilobular portion of the lobule
✓ Upper lobe predominance and uneven
distribution
✓ Strongly associated with smoking
EMPHYSEM
A
34.
Panlobular emphysema
✓ Affectsthe whole secondary lobule
✓ Lower lobe predominance
✓ In alpha-1-antitrypsin deficiency, but also seen i
n
smokers with advanced emphysema
35.
Paraseptal emphysema
✓ Adjacentto the pleura and interlobar fissures
✓ Can be isolated phenomenon in young adults, or i
n
older patients with centrilobular emphysema
✓ In young adults = spontaneous pneumothorax
36.
Lung cysts: Radiolucentareas with wall thickness
of less than 4mm
Cavities -Radiolucent areas with wall thickness of
more than 4mm and are seen in infection (TB,
Staph, fungal, hydatid), septic emboli, squamous
cell carcinoma and Wegener's disease
CYSTIC LUNG DISEASE
Bronchiectasis is definedas localized bronchial dilatation
Bronchial dilatation (signet-ring sign)
Bronchial wall thickeningLack of normal tapering with
visibility of airways in the peripheral lung
Mucus retention in the bronchial lumen
Associated atelectasis and sometimes air trapping
A signet-ring sign represents an axial cut of a dilated
bronchus (ring) with its accompanying small artery (signet)
BRONCHIECTASI
S
39.
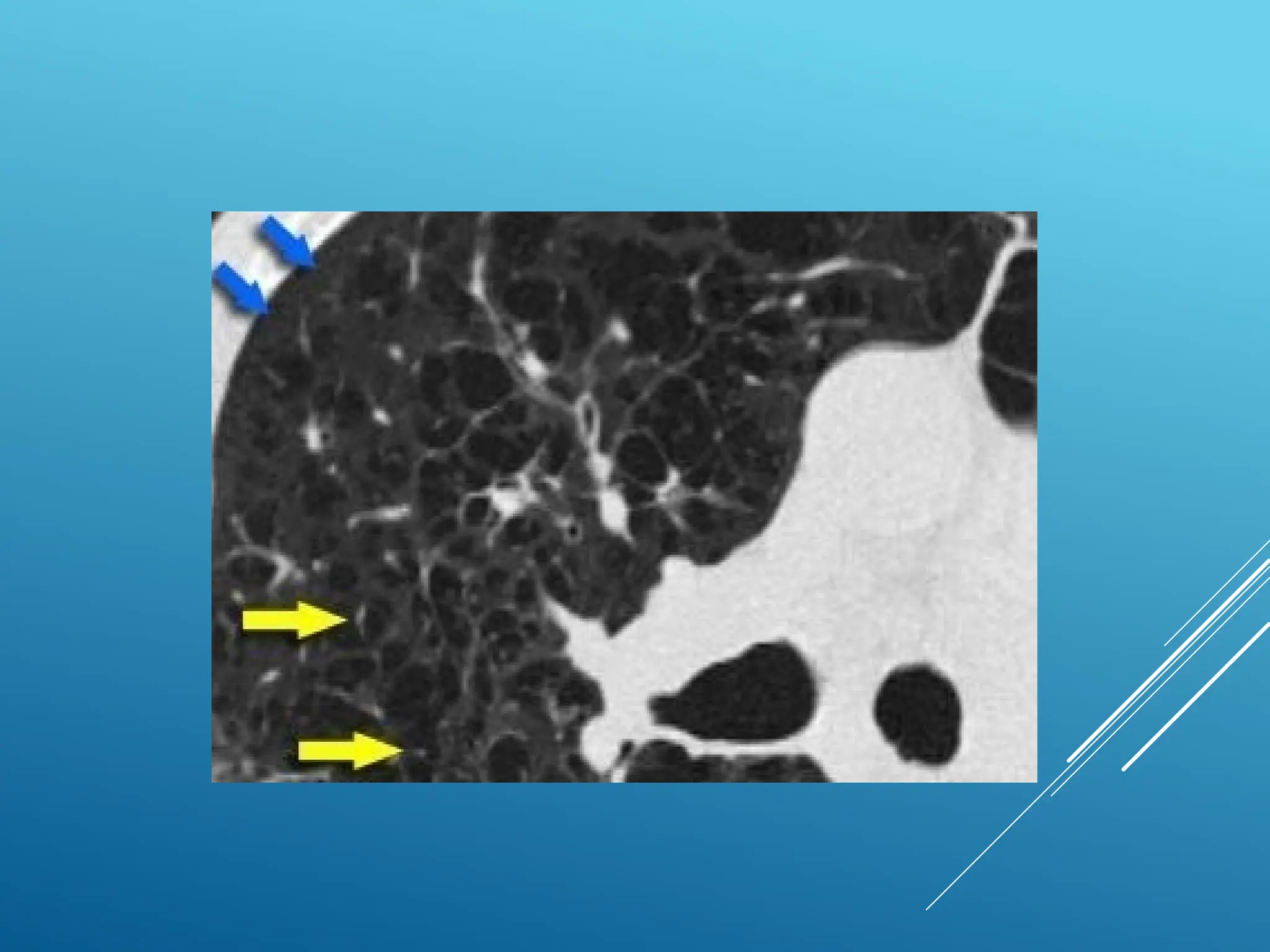
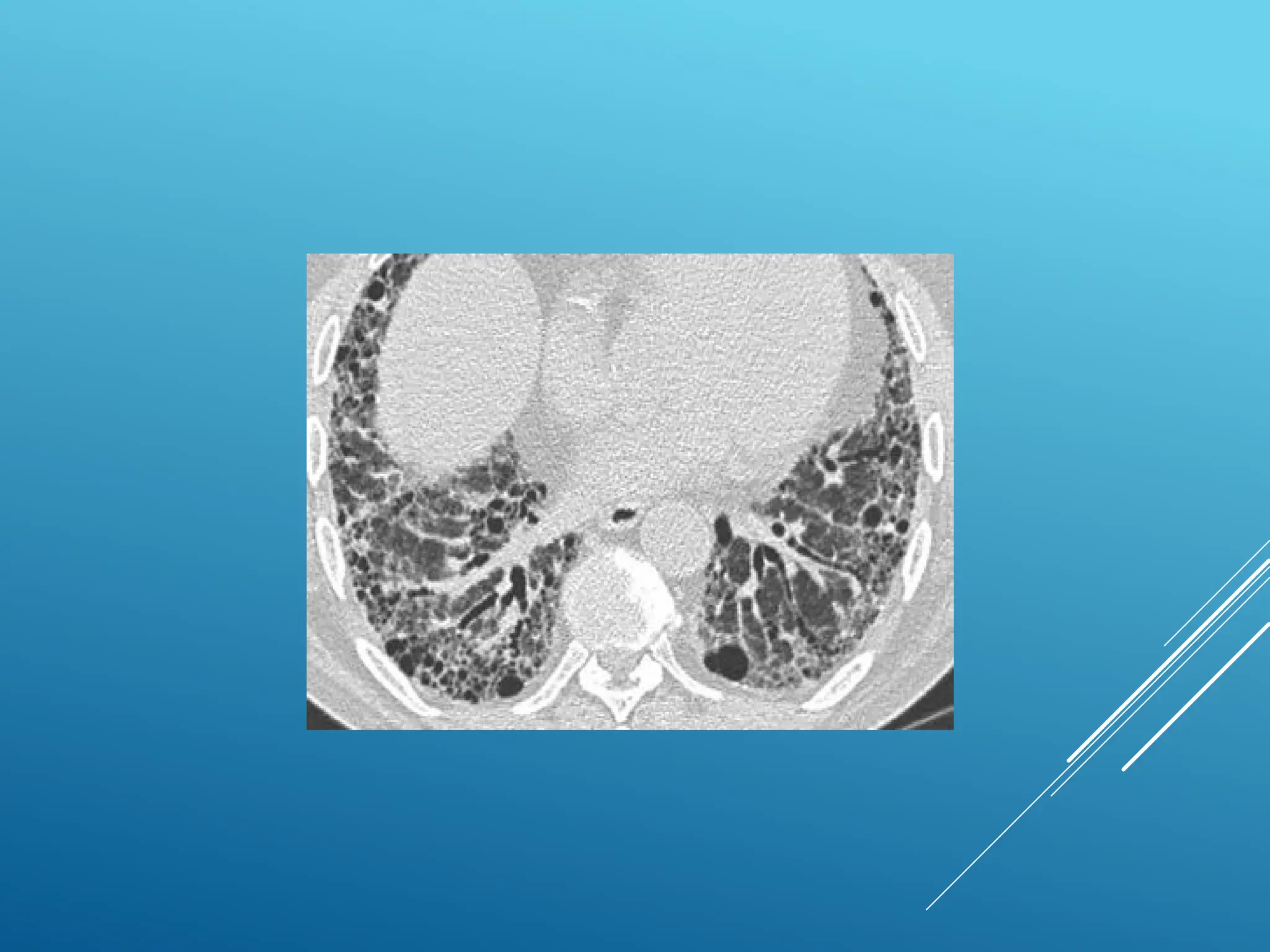
Honeycombing is definedby the presence of small
cystic spaces with irregularly thickened walls
composed of fibrous tissue
Predominate in the peripheral and subpleural lung
regions
Subpleural honeycomb cysts occur in several
contiguous layers
HONEYCOMBI
NG
IDIOPATHIC INTERSTITIAL
PNEUMONIAS
Also aregroup of diseases with predominantly reticular or linear
pattern of opacities. Most common in the group is known as Idiopathic
Pulmonary Fibrosis.
In the past, the lack of standarised international classification resulted in
variable and confusin diagnostic criteria and terminology.
An international consensus statement defining the clinical, pathology and
radiological features of patients with IIP was adopted by American
throracic society and European Respiratory society in 2001. Revised in
2013.
The ATS/ERS classification classified it into 7 categories.
46.
IDIOPATHIC INTERSTITIAL FIBROSIS
(IDIOPATHICPULMONARY FIBROSIS)
Most common
It is the term used for clinical syndrome associated with
morphological pattern of UIP.
Clinically-
M>F ( slightly), usually older than 50 years, smoker.
Progressive dyspnea , cough, F/O right heart failure
Median survival time after diagnosis- 2.5-3.5 years.
HRCT-
Bilateral , patchy,subpleural ,
basilar reticular opacities
Presence of apicobasal
gradient
Associated with architectural
distortion, honeycombing and
traction bronchiectasis.
GGO may be seen, less
prominent than reticular
opacities.
49.
Levels of certaintywith HRCT
Diagnostic features of UIP-
Reticular opacities and traction
bronchiectasis
Honeycombing ( critical for
diagnosis)
Subpleural and basal
distribution
Architectural distortion from lung
fibrosis
Absence of inconsistent features.
Heterogenous area with regions of
fibrotic lung alternating with normal
lung
UIP pattern in HRCT correlates with
UIP pattern at surgical lung biopsy
Inconsistent features
Upper or mid lung predominance
Peribronchovascular predominance
Extensive ground glass
Multiple micronodules
Discrete cysts
Consolidation
Mosaic attenuation
Possible UIP
Reticular opacities often associated with traction
bronchiectasis.
Distribution subpleural and basal
Absence of inconsistent features
Absence of honeycombing.
51.
NONSPECIFIC
INTERSTITIAL
PNEUMONIAS
Very good prognosisand responds well to steroid treatment.
Although called idiopathic, morphological pattern is associated with patterns
in connective tissue disorders, drug induced pneumonitis, hypersensetive
pneumonitis, infection and immunodificiency. Once the pattern of NSIP has
been determined, secondary forms of NSIP should be excluded out by clinician.
Clinical-
F>M, smokers and nonsmokers both, 40-50 years ( decade younger than patients
with UIP)
Dyspnea, cough and weight loss
52.
• Histologically-
Temporally and
histologicallyhomogenous
lung involvement ( key
differentiating feature
from UIP)
Xray-
Initially normal, later Reticular
opacities in lower lobes without
honeycombing
No apicobasal gradient
53.
HRCT-
Bilateral , predominantlylower lobes, subpleural,
symmetricity.
Traction bronchiectasis
Volume loss
No honeycombing or microcystic honeycombing (
in comparision to macrocystic honeycombing in
UIP)
Ground Glass opacities are the predominant
feature (50% cases).
Prognosis – Good
Steroid responsive
5 year mortality rate <18 percent.
CRYPTOGENIC ORGANISING
PNEUMONIA
Previously calledBronchiolitis Obliterans Organizing Pneumonia (BOOP).
A non specific inflammatory response by the lung to various forms of injury.
Inflammatory process where the healing process is characterized by the
organization of the exudate rather than by resorption( unresolved pneumonia).
Clinical-
Mild SOB, fever, cough, chills, weight loss, myalgia.
Most are non smokers and most respond to
steroids. male= females, onset: 55yrs.
Most patients report respiratory tract infection
preceeding the illness.
• As with other interstitial pneumonias, pattern may occur in a wide variety of
entities, notably collagen vascular disease, infectios, hence final diagnosis should
be rendered only after exlusion of differntials.
56.
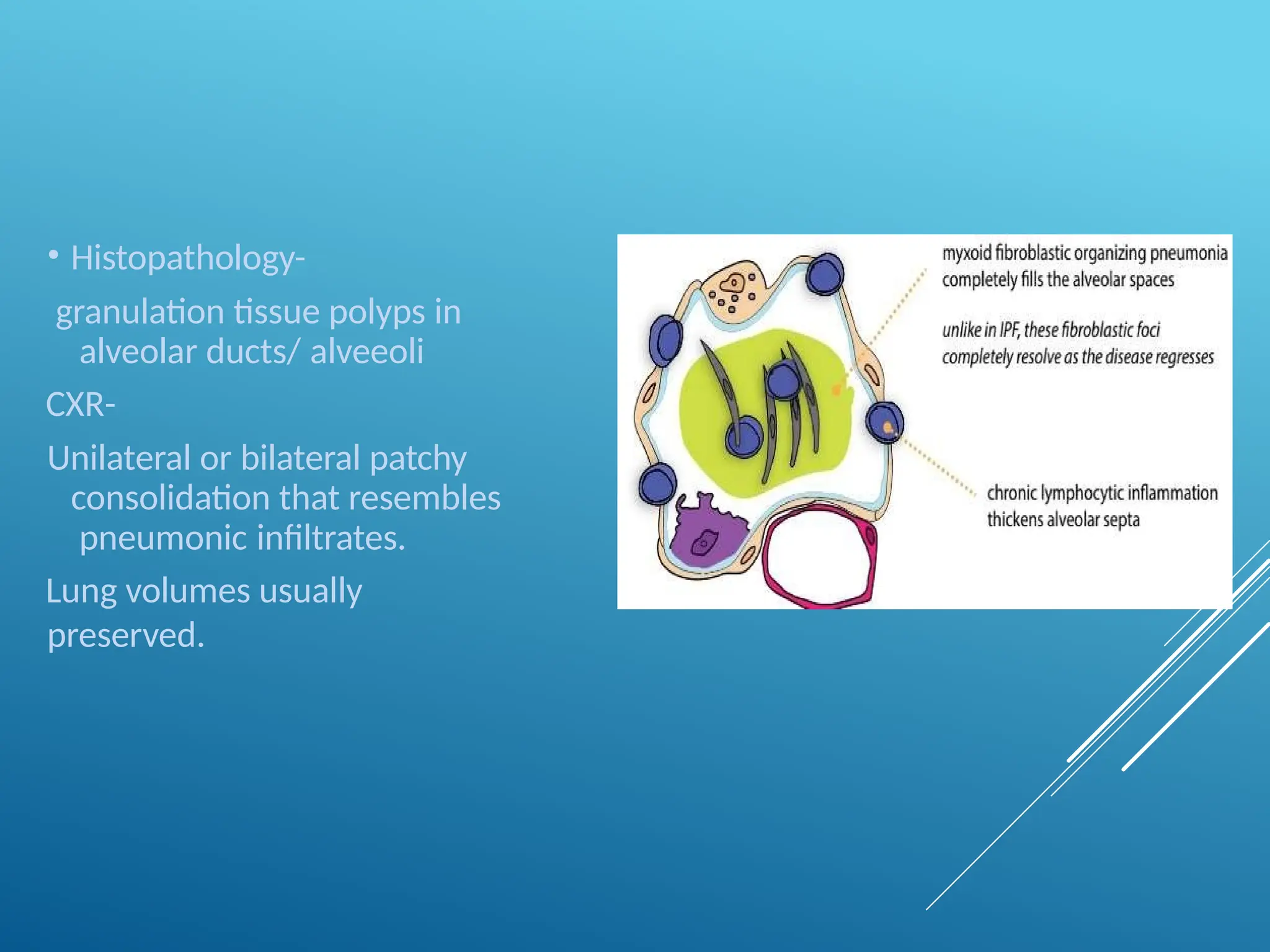
• Histopathology-
granulation tissuepolyps in
alveolar ducts/ alveeoli
CXR-
Unilateral or bilateral patchy
consolidation that resembles
pneumonic infiltrates.
Lung volumes usually
preserved.
57.
CT findings moreextensive than expected from Xray
Characteristic peripheral and peribronchial distribution
Lower lung lobes more involved.
In some cases, outermost subpleural areas spared.
Lung opacities range from GGO to consolidation.
Opacities have tendency to migrate with change in
location and shape even without treatment.
In appropriate clinical setting, consolidation that
increases over several weeks despite antibiotics may be
suggestive.
Reverse halo sign- specific finding in COP. (20% cases)
Crazy paving pattern ( infrequent).
Atypical findings include- irregular linear opacities,
solitary focal lesions, multiple nodules with cavitations.
59.
RESPIRATORY BRONCHIOLITIS
RELATED INTERSTITIALLUNG DISEASE
(RB-ILD)
Very small percentage of typically young heavy smokers.
exclusively in current or former cigarette smokers
30 to 40 years old
male-to-female ratio of 2:1.
Symptomatic with decreased diffusing capacity.
RB-ILD have good prognosis following smoking cessation.
No arbitrary cut off between RB and RB-ILD on HRCT.
Chest radiographic -thickening of the walls of the central and
peripheral bronchi and diffuse bilateral reticulonodular opacities.
normal in 20% of patients
60.
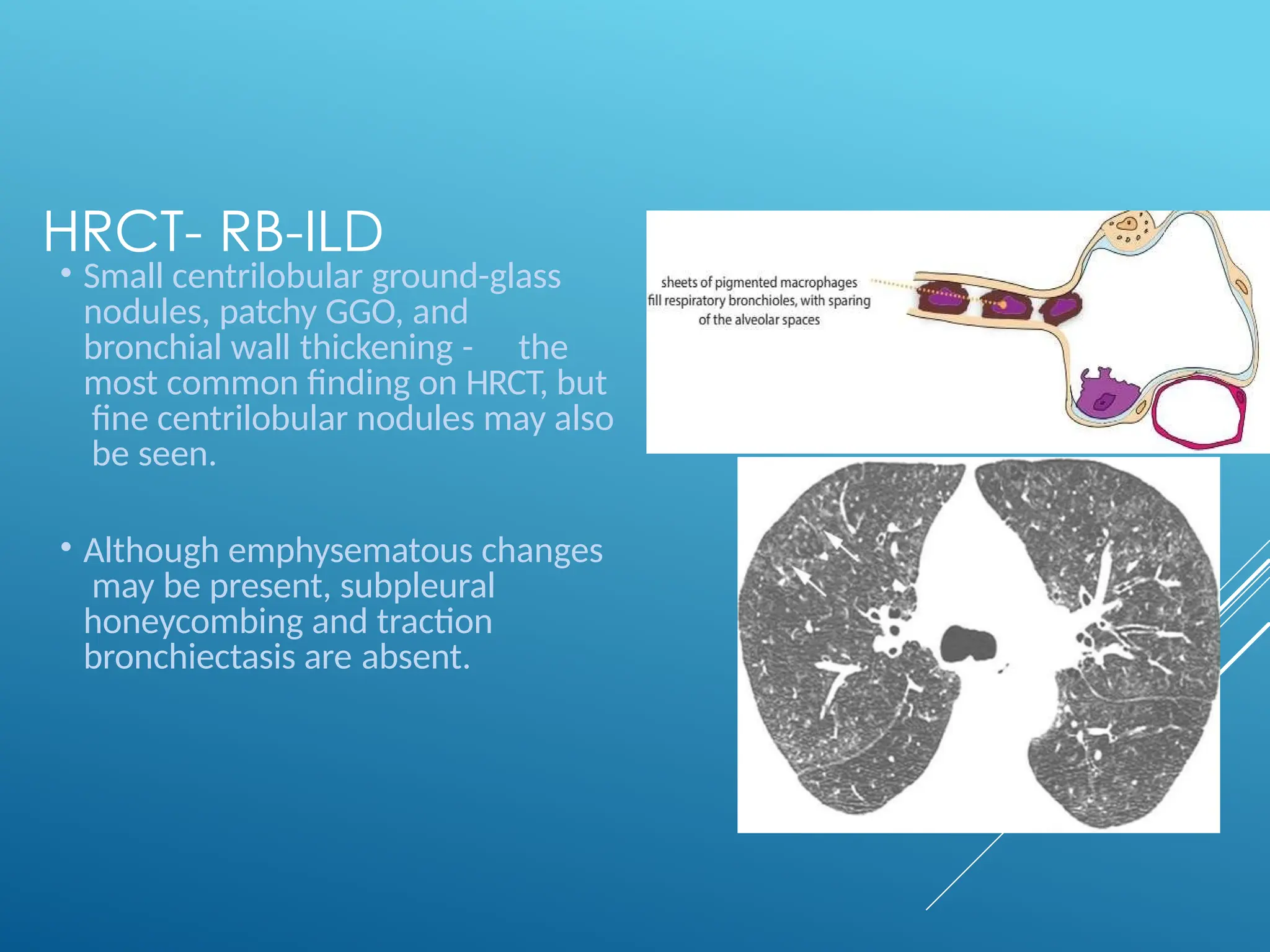
HRCT- RB-ILD
• Smallcentrilobular ground-glass
nodules, patchy GGO, and
bronchial wall thickening - the
most common finding on HRCT, but
fine centrilobular nodules may also
be seen.
• Although emphysematous changes
may be present, subpleural
honeycombing and traction
bronchiectasis are absent.
61.
DESQUAMATIVE
INTERSTITIAL
PNEUMONIA
Rare , stronglyassociated with cigarette
smoking.
Clinical- 30-40 years, male , smoker, average
smoking
Clin/path/rad distinction between RBILD and
DIP blurred but 6-30% mortality
Ground glass more extensive and diffuse as
compared to RB-ILD, may be subpleural
and basal. Centrilobular nodules
uncommon.
Mid and lower lungs predominately involved
with a peripheral predilection.
–/+ reticulation, cysts, emphysema
62.
ACUTE INTERSTITIAL
PNEUMONIAS
Only entityin IIP with acute onset of
symptoms.
Rapidly progressive interstitial pneumonia
with poor prognosis
Histologically – diffuse alveolar damage,
hyaline membrane formation and
indistinguishable from ARDS.
Clinical-
Mean age – 50 years, M=F.
Preceeding flu like illness followed by rapidly
progressive dyspnea in few weeks.