Downloaded 452 times
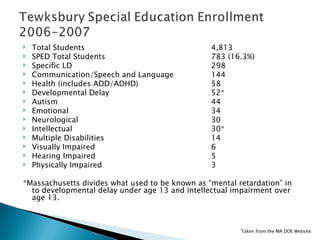
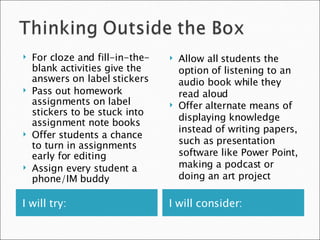

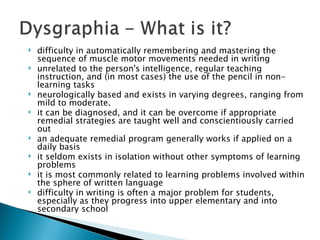
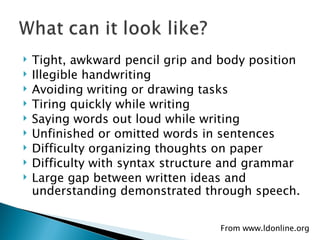
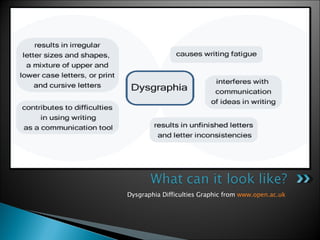









The document provides information about professional development training sessions for teachers on learning disorders. It includes an agenda for two training sessions that will cover various topics like specific learning disabilities, speech/language impairments, and instructional strategies. Participant goals include gaining knowledge of learning disorders and applying differentiated instructional approaches. The document also provides demographic data on students with disabilities in the school district and strategies teachers can use to support students with different types of learning disabilities or difficulties.
















![An Auditory Learner Is Someone Who[1]](https://cdn.slidesharecdn.com/ss_thumbnails/anauditorylearnerissomeonewho1-091023155804-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























































































