Download as PDF, PPTX
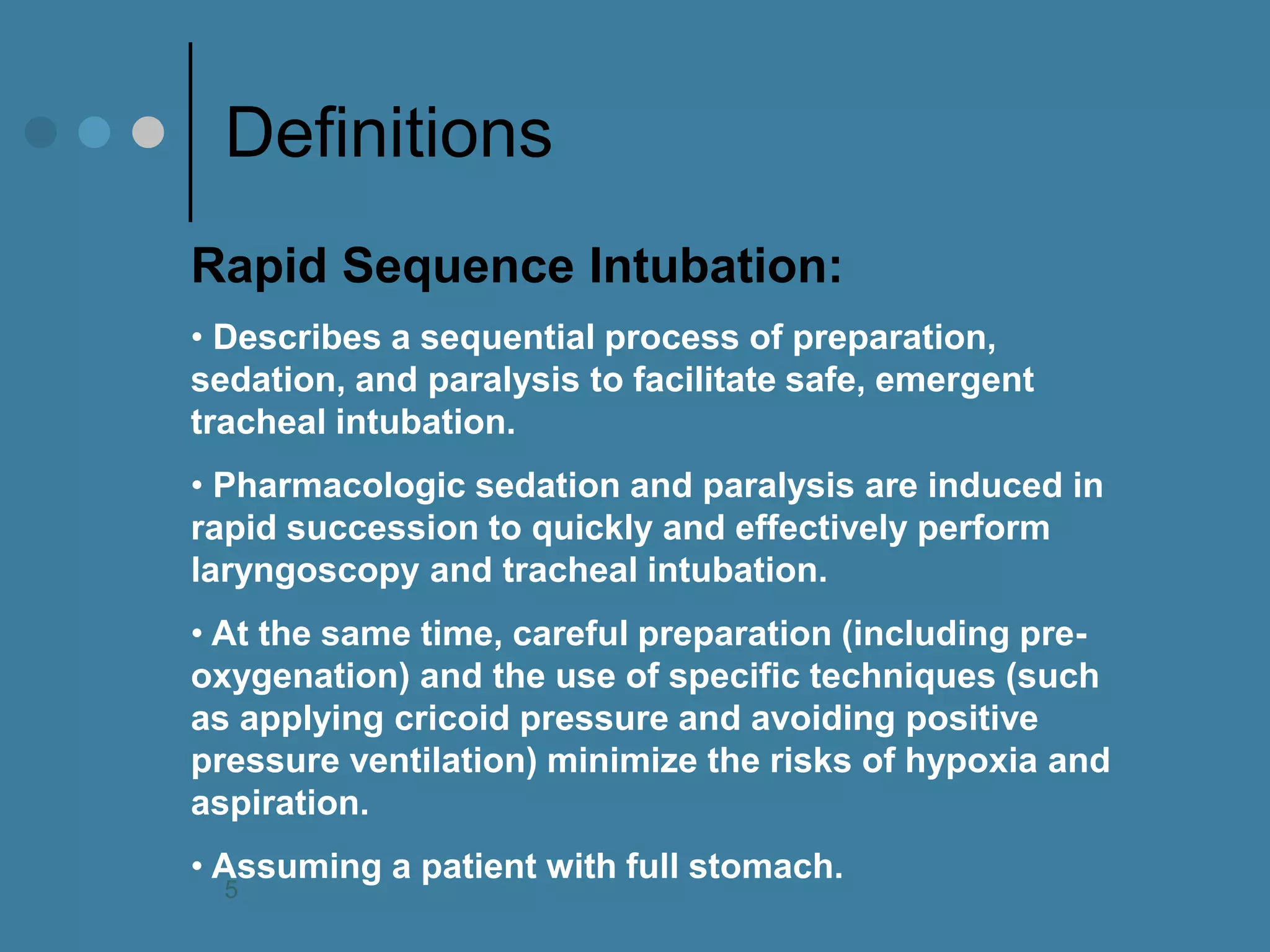
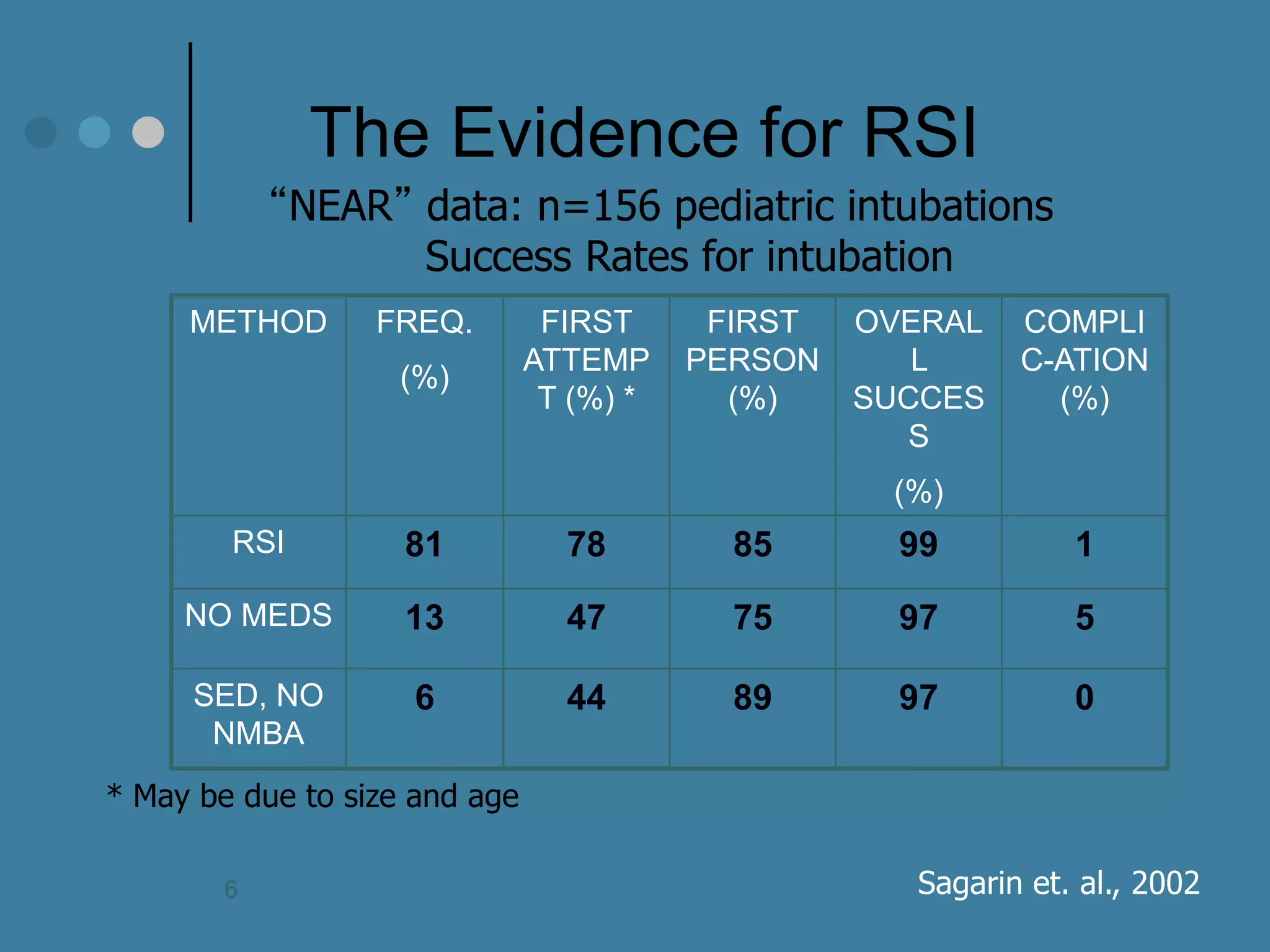
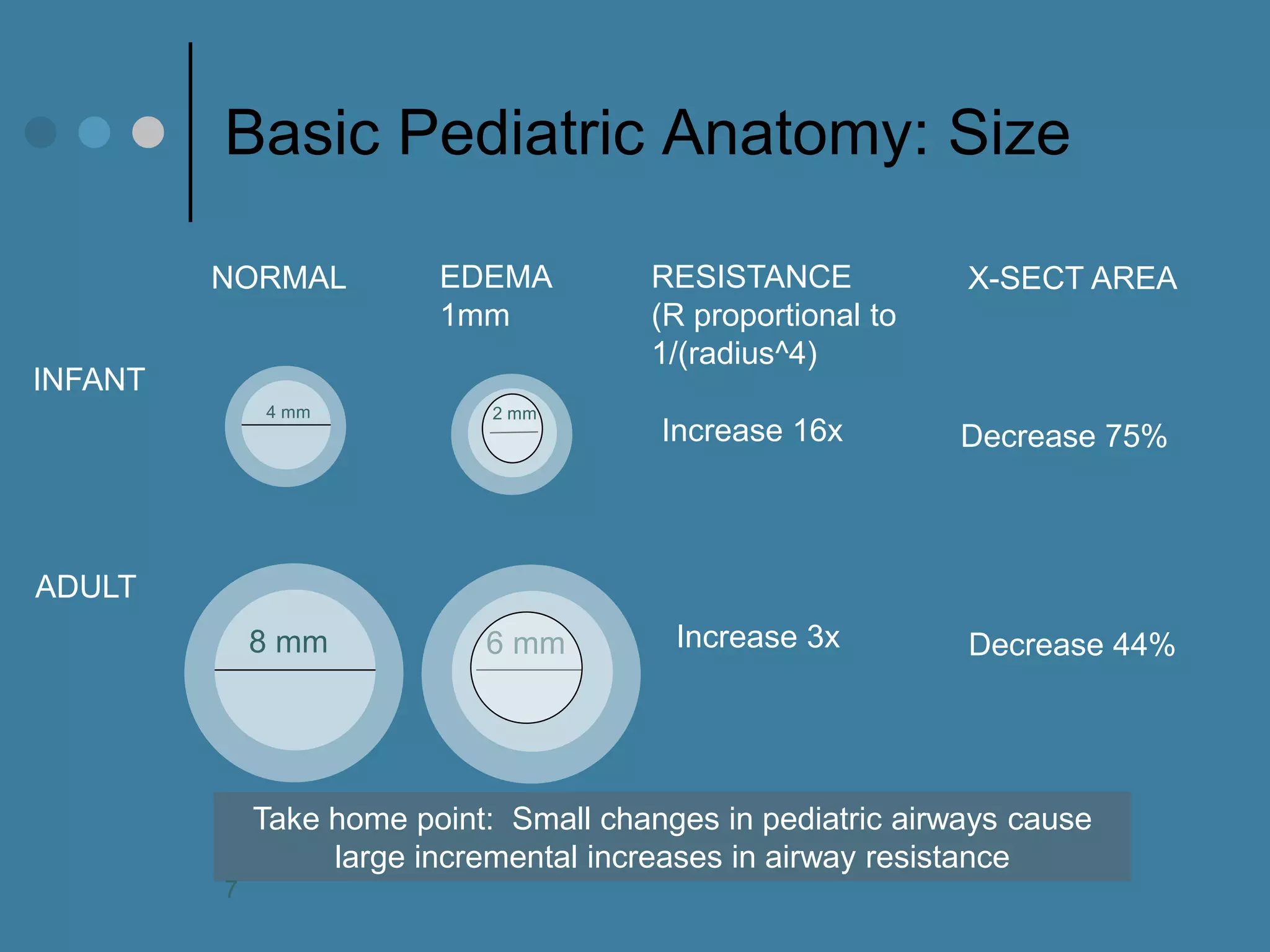
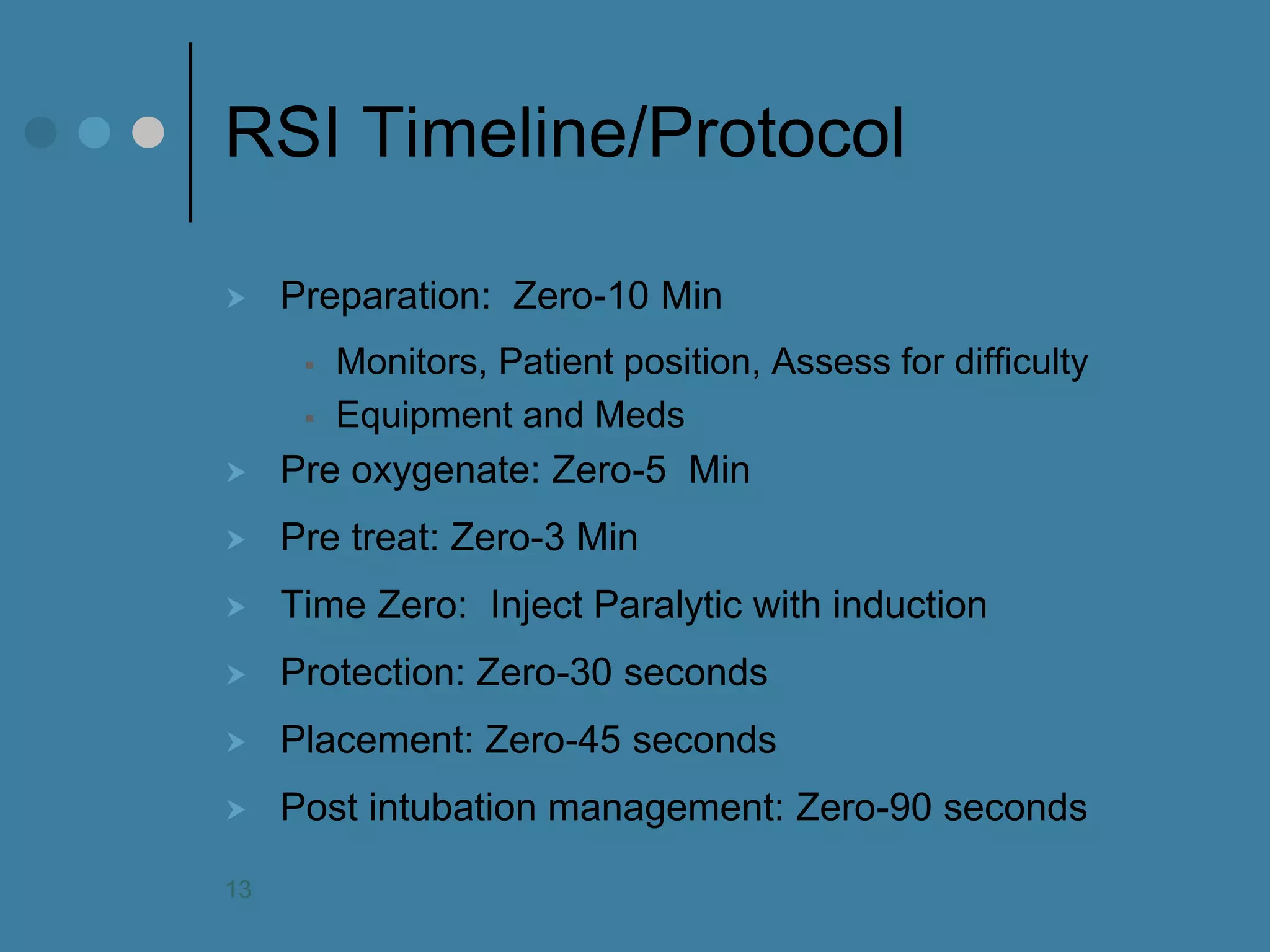
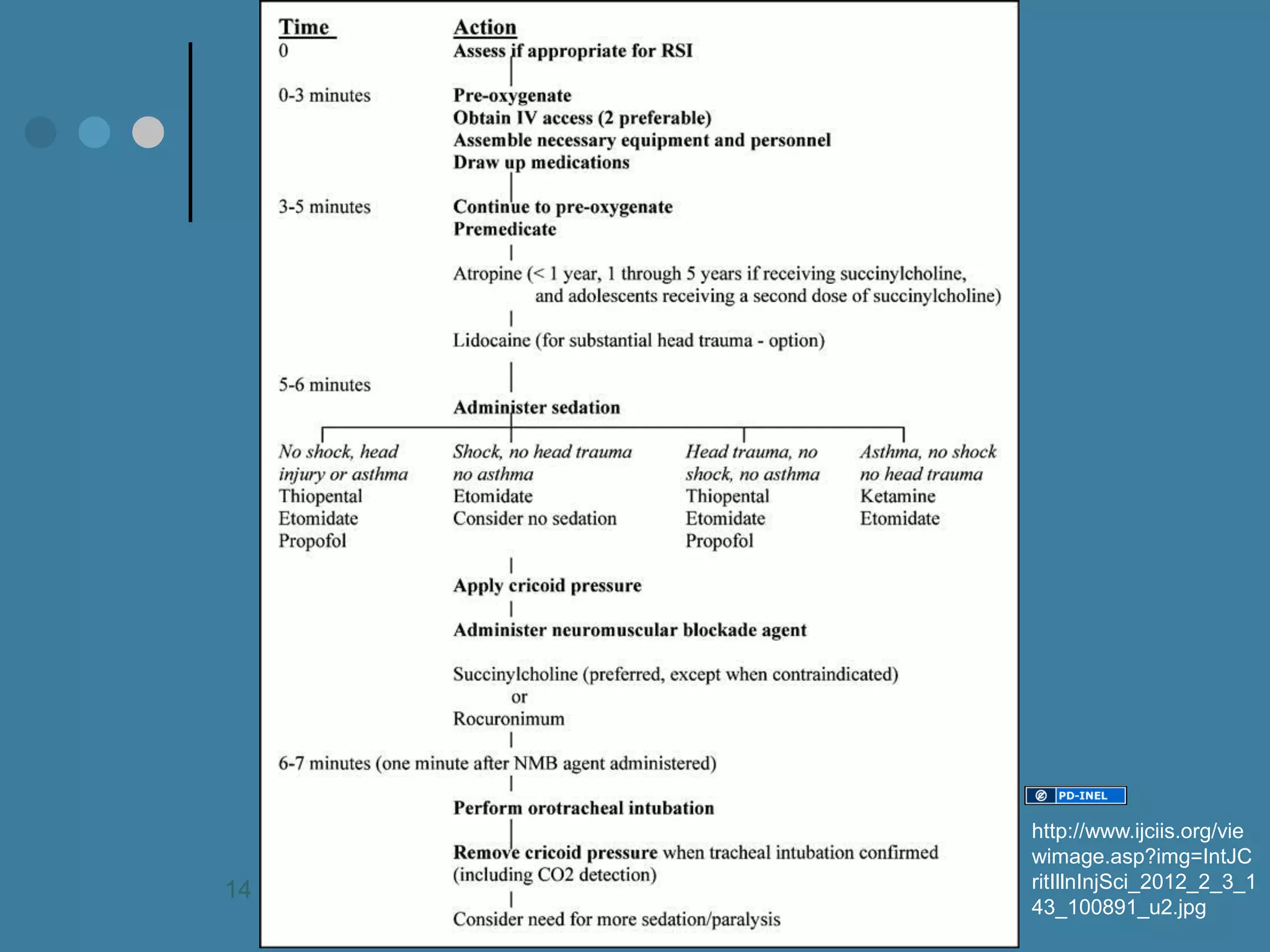
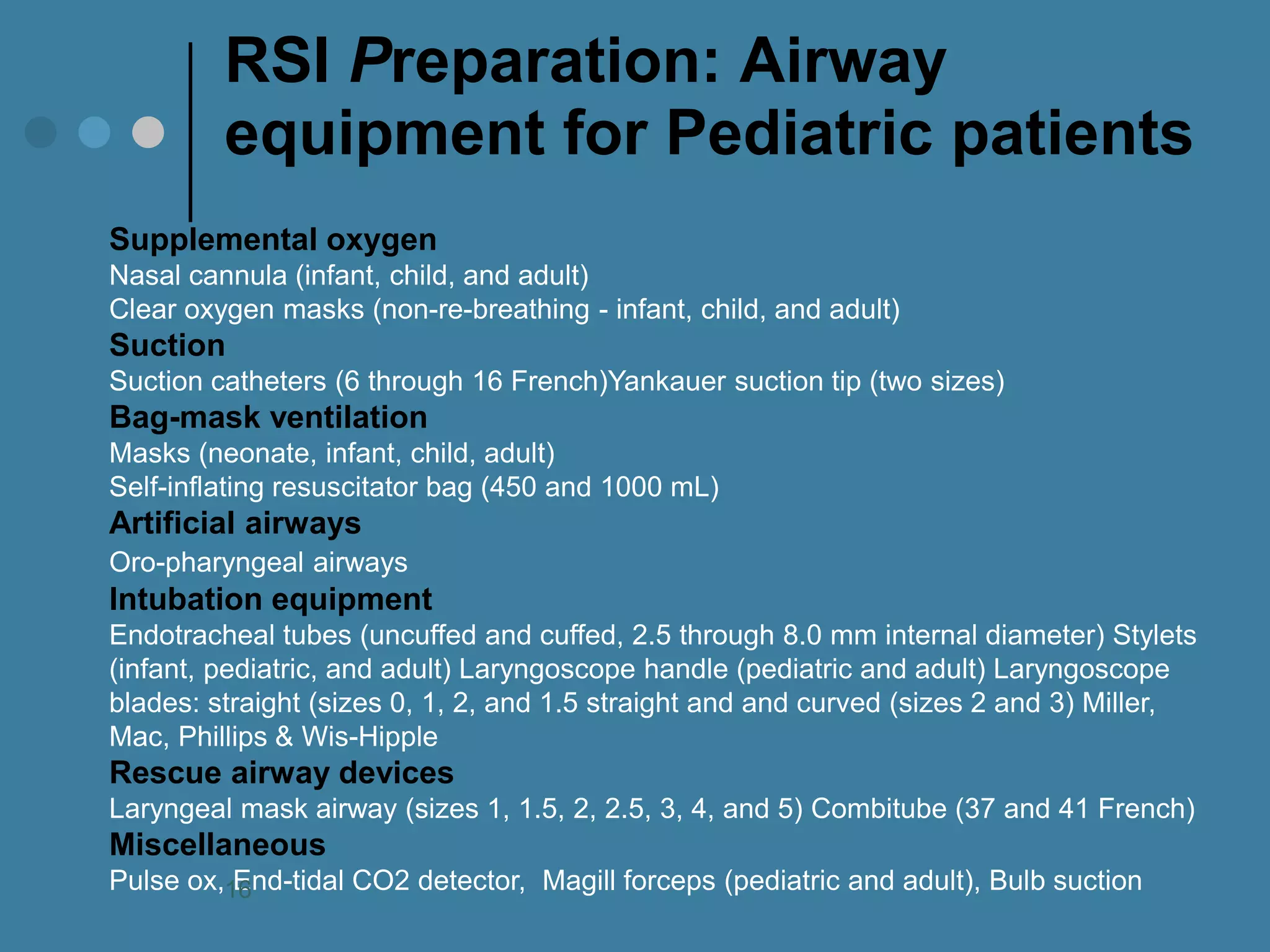

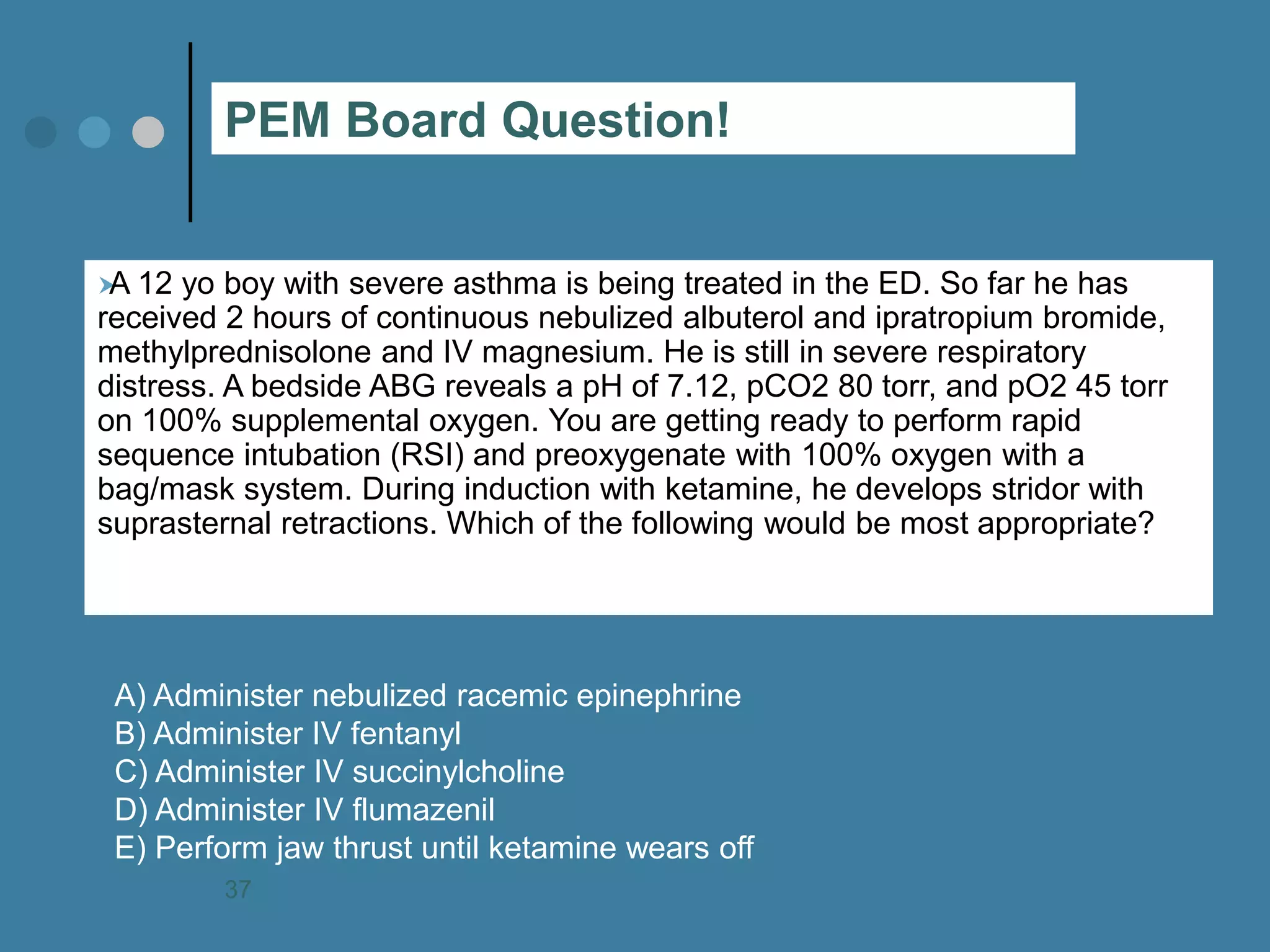

This document discusses Rapid Sequence Intubation (RSI) and emergency airway support specifically for pediatric patients in emergency medicine. It provides details on the objectives, procedures, pharmacology, equipment, and assessments necessary for successful RSI, highlighting the importance of preparation and knowledge of pediatric airway anatomy. The content aims to educate healthcare professionals on effective methods for managing pediatric intubations in emergency situations.











































































































