Download as PDF, PPTX
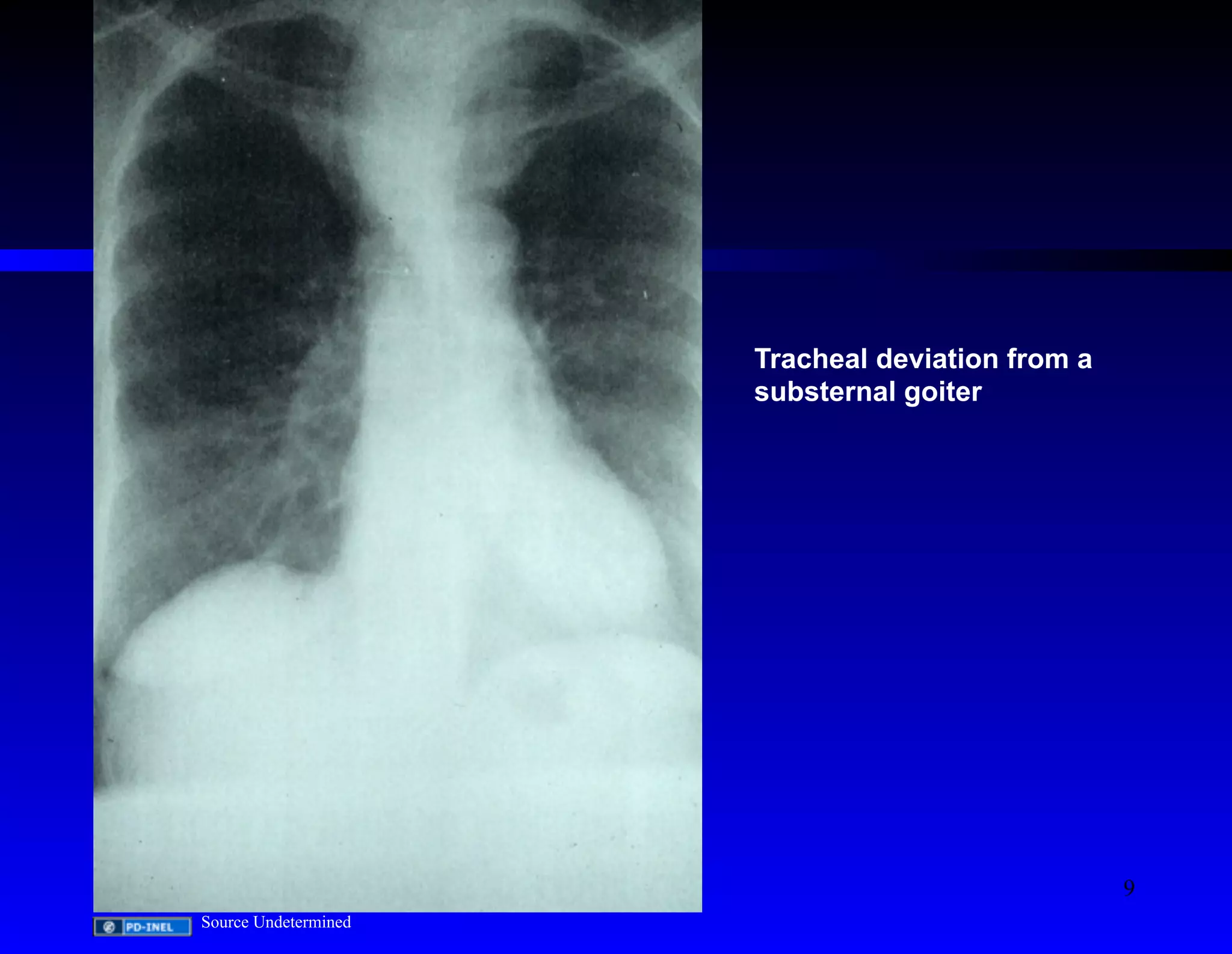
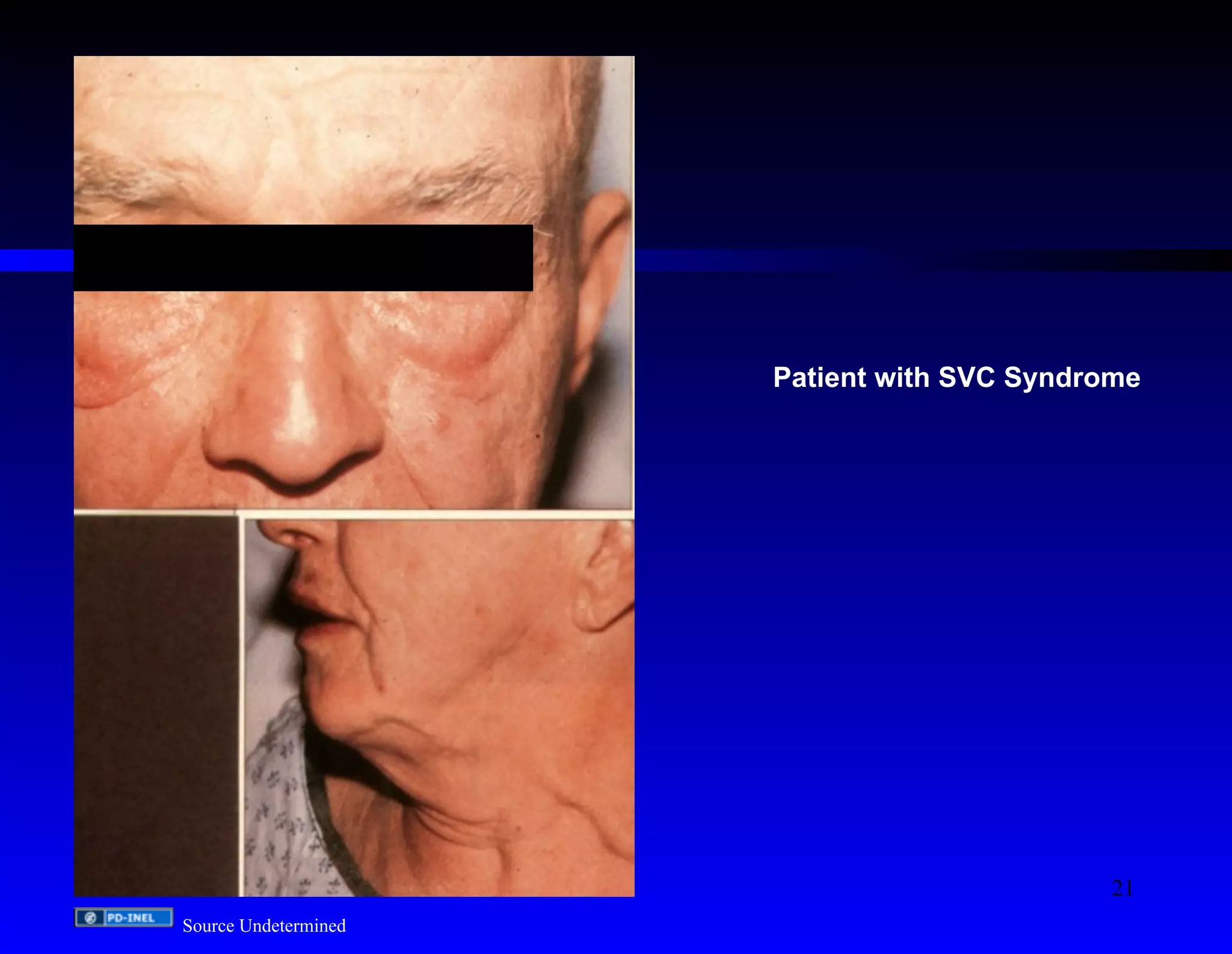
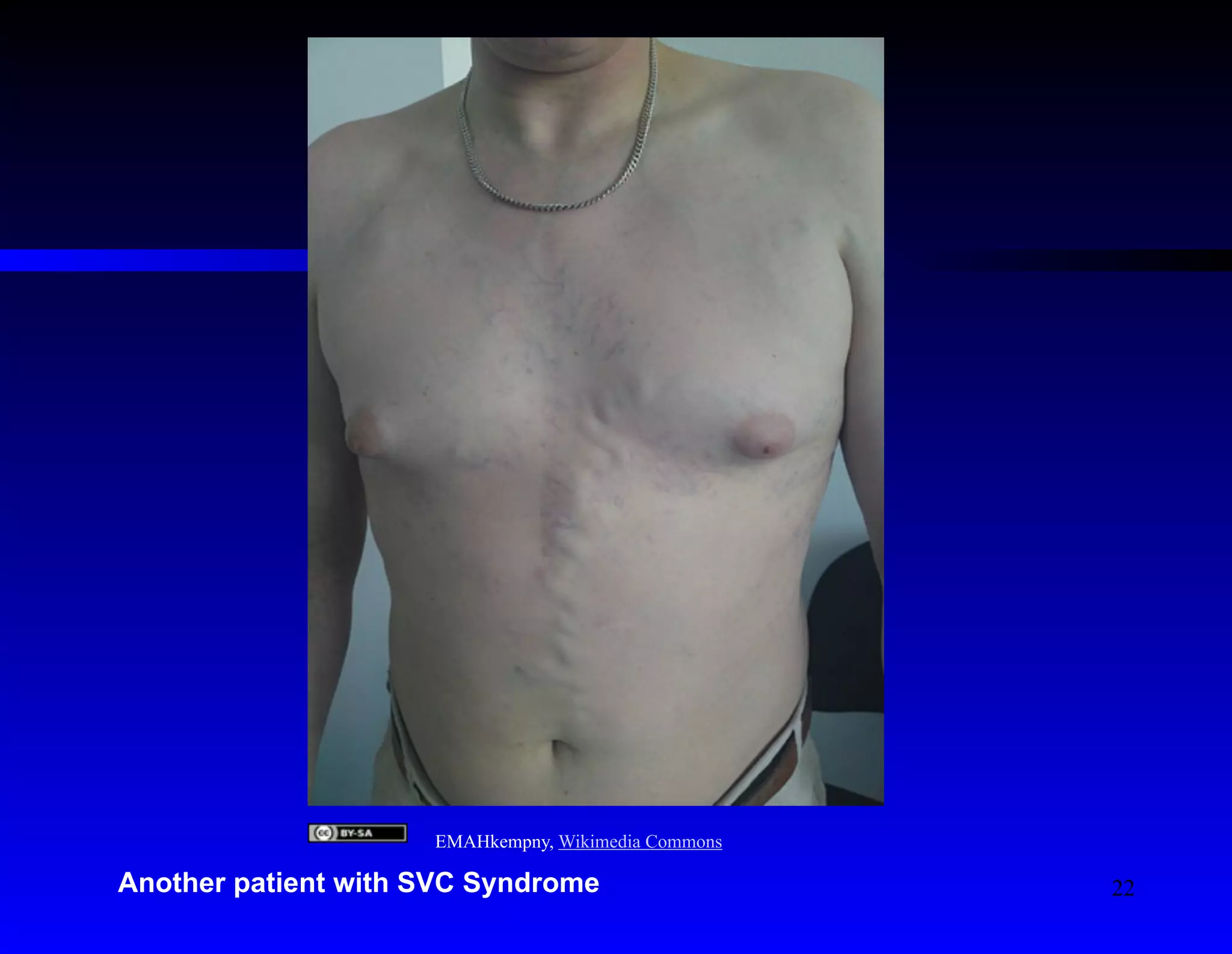
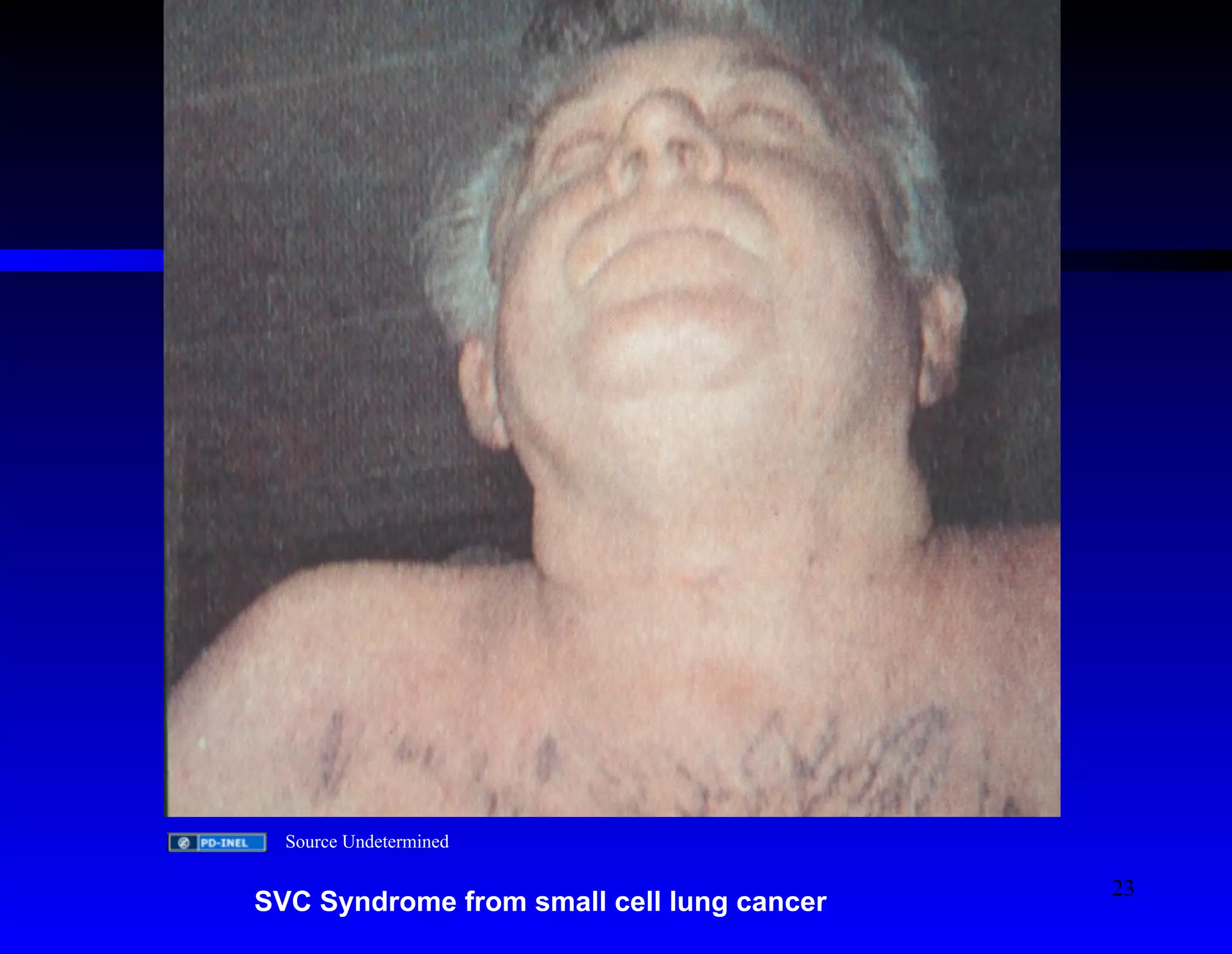
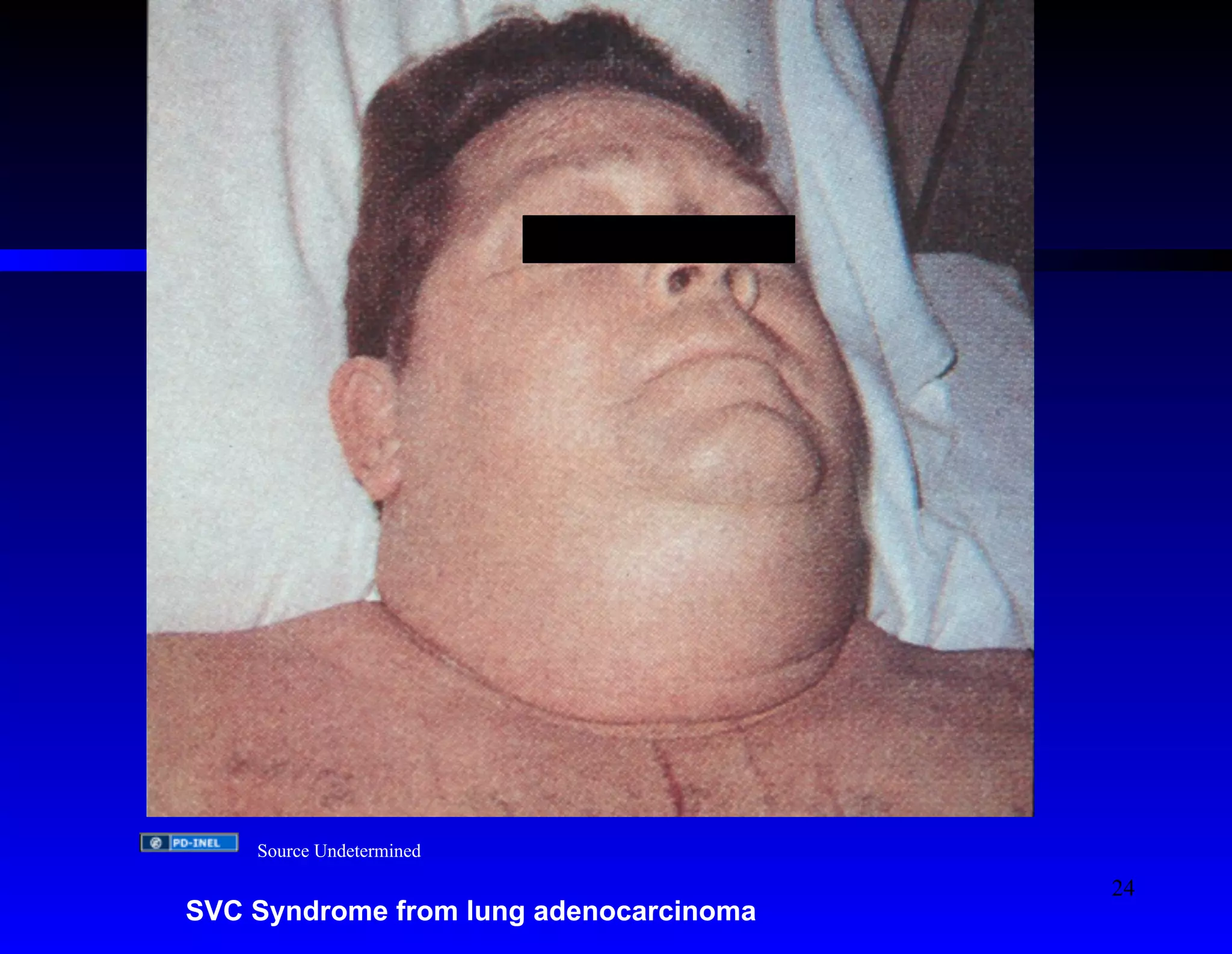


The document discusses oncologic emergencies, highlighting that malignancy is the second leading cause of death in the U.S. and the treatment of complications can significantly improve patient outcomes. It lists major emergency complications such as upper airway obstruction, malignant pericardial tamponade, and hypercalcemia, while detailing their symptoms, diagnosis, and treatment options. The content also emphasizes the importance of proper medical intervention and the potential for life-saving procedures in managing these emergencies.























































































