Downloaded 274 times


























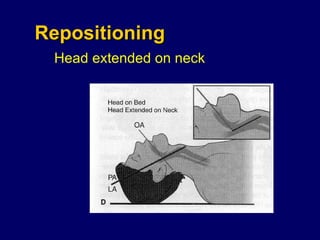
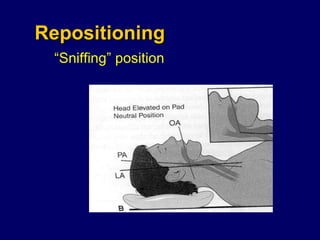










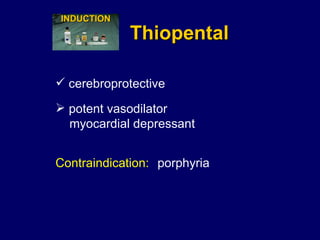
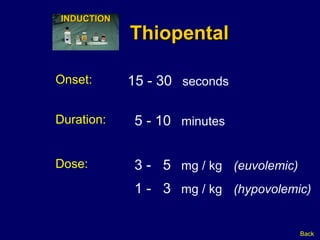

















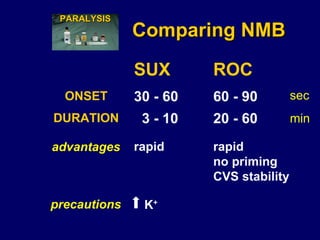






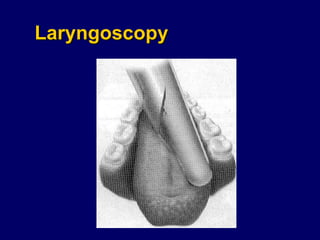

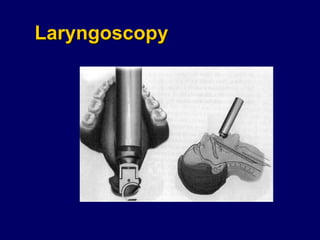



























The document summarizes key points from an emergency medicine seminar on airway management and intubation. It discusses indications for intubation, preparing for difficult airways and mask ventilation, techniques for rapid sequence intubation including preoxygenation and induction agents, and considerations when choosing between succinylcholine and rocuronium as paralytic agents. Case examples are provided to demonstrate how to assess indications and choose an approach for different patients requiring emergency intubation.























































































