Downloaded 34 times
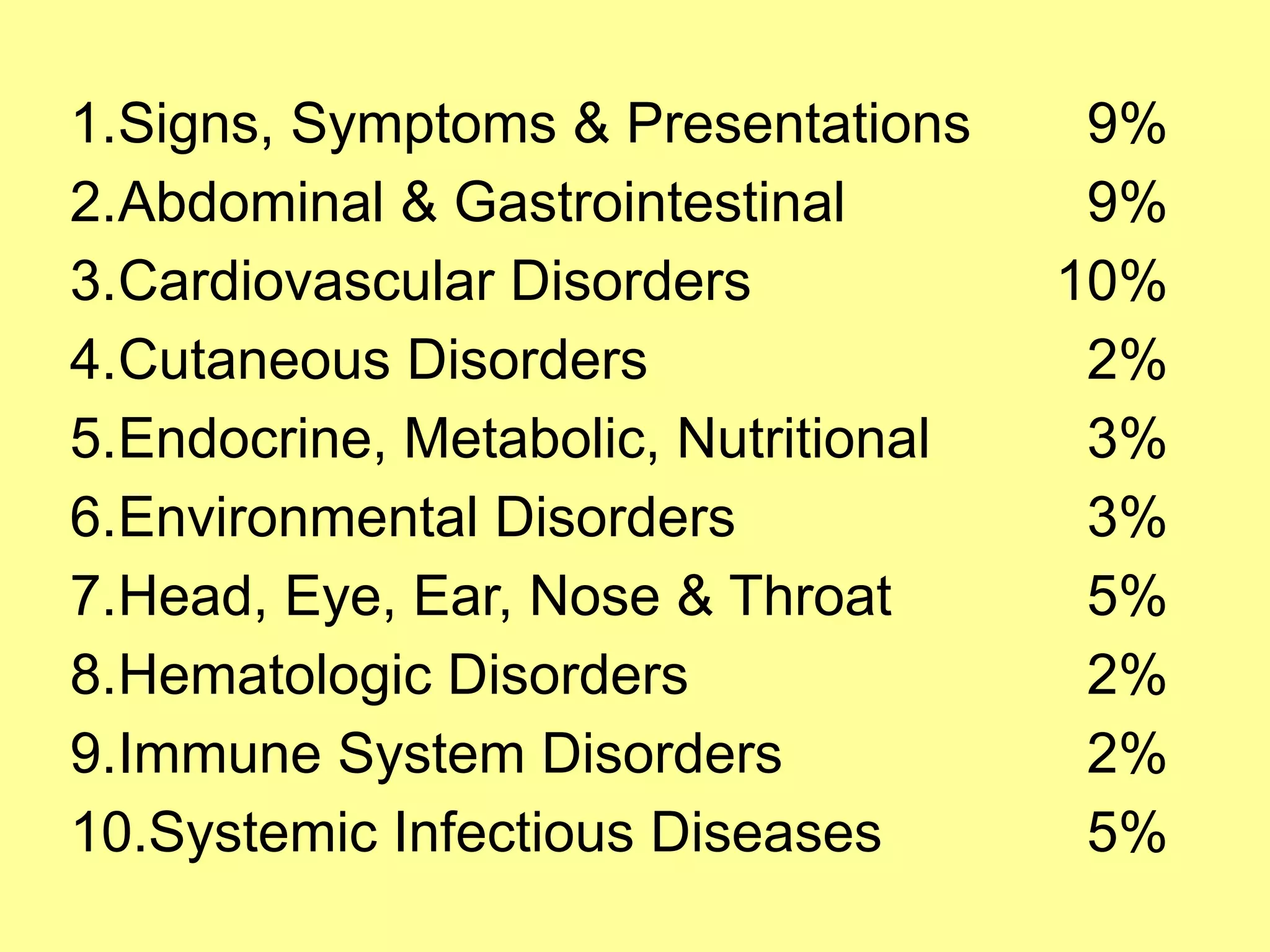
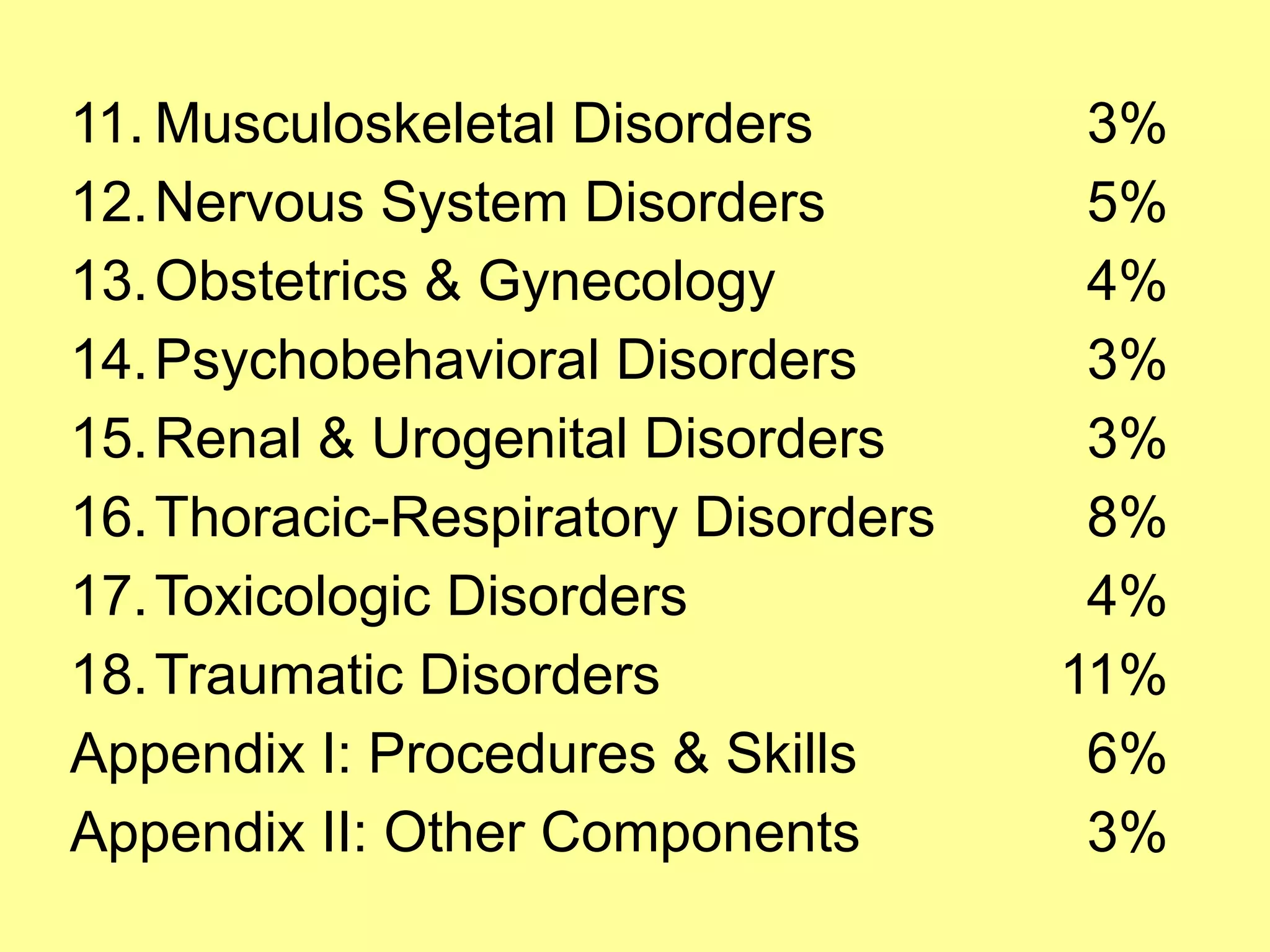
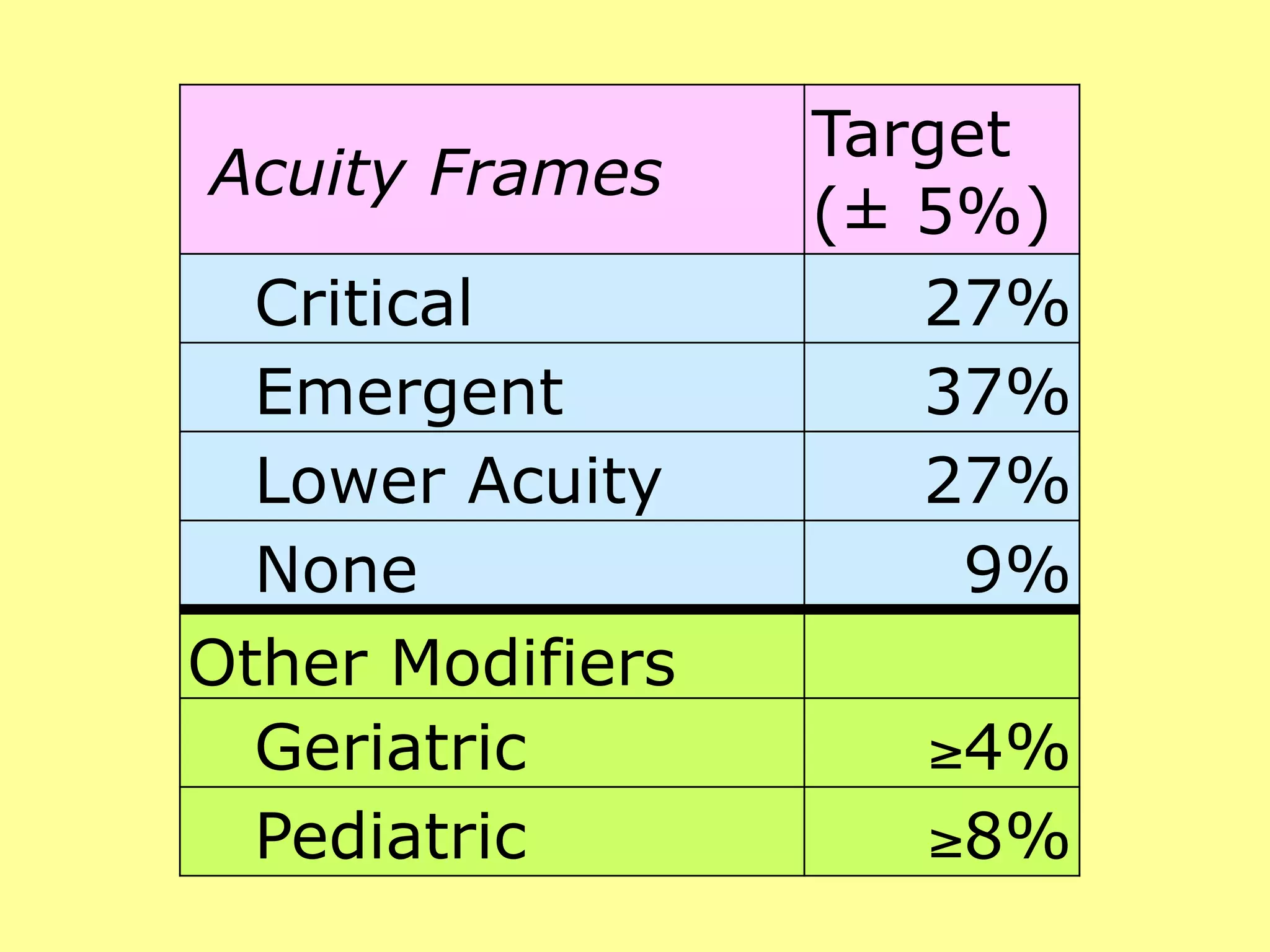
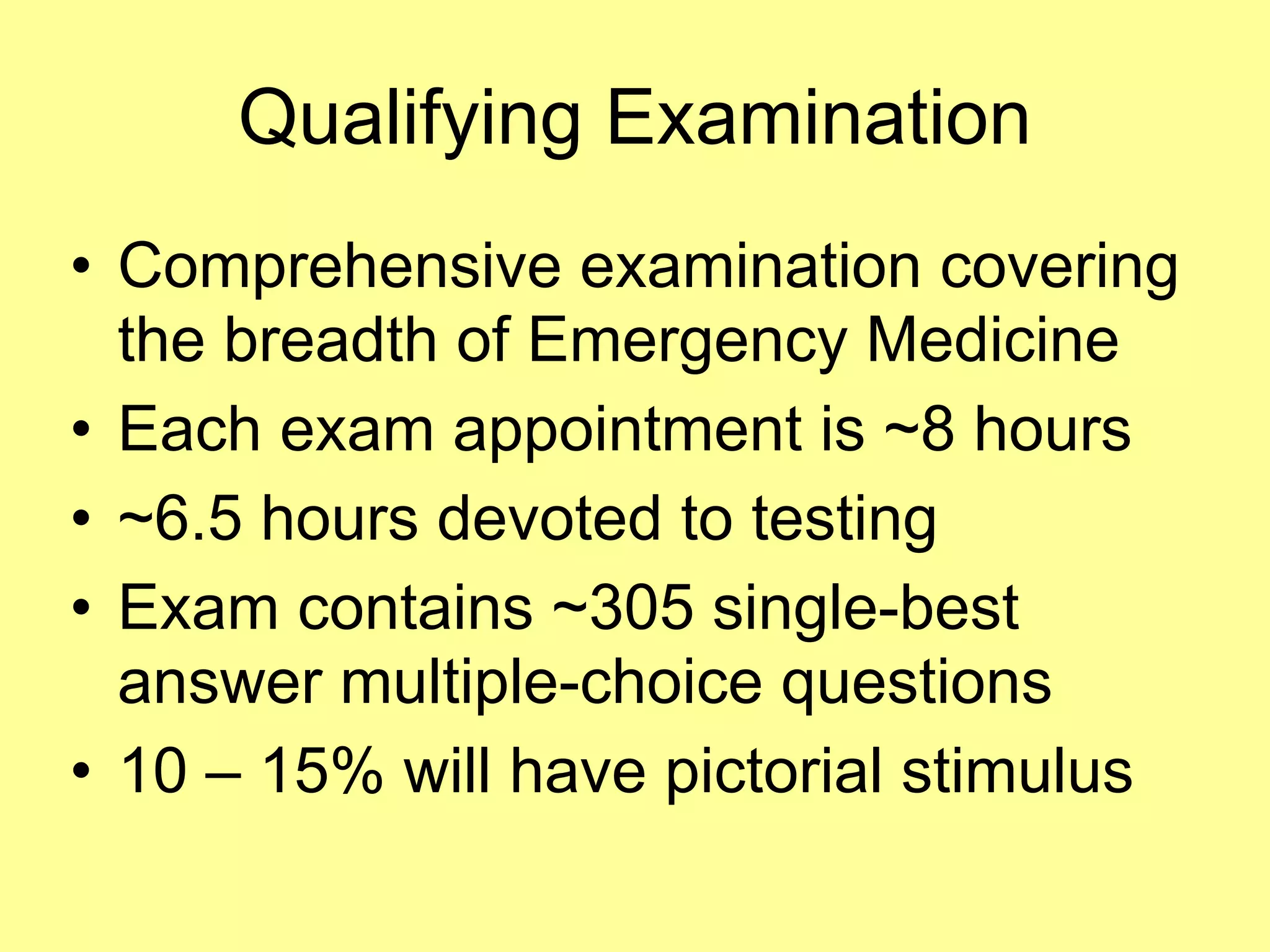


This document provides guidance on test-taking skills specifically for emergency medicine examinations. It emphasizes the importance of understanding the structure and content of tests, strategies for answering questions, and addressing test anxiety. The author, Joe Lex, offers practical tips to improve test performance and highlights the significance of preparation and confidence.



































































