Download as PDF, PPTX


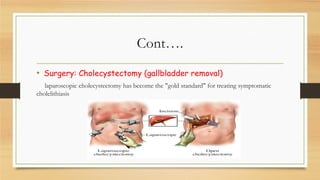
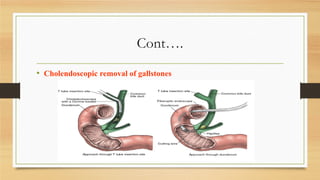
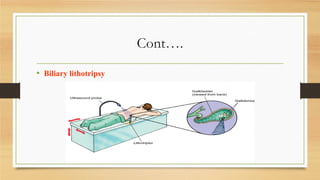

Mr. B, a middle-aged man, experienced abdominal pain after eating fatty foods that radiated to his back and caused nausea. An examination and ultrasound were planned to evaluate for possible biliary diseases like cholelithiasis. Cholelithiasis, or gallstones, occur when bile contains too much cholesterol and not enough bile salts, causing stones to form in the gallbladder or ducts. Gallstones are often diagnosed by ultrasound and may be treated by laparoscopic cholecystectomy to remove the gallbladder.






































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




