Downloaded 663 times





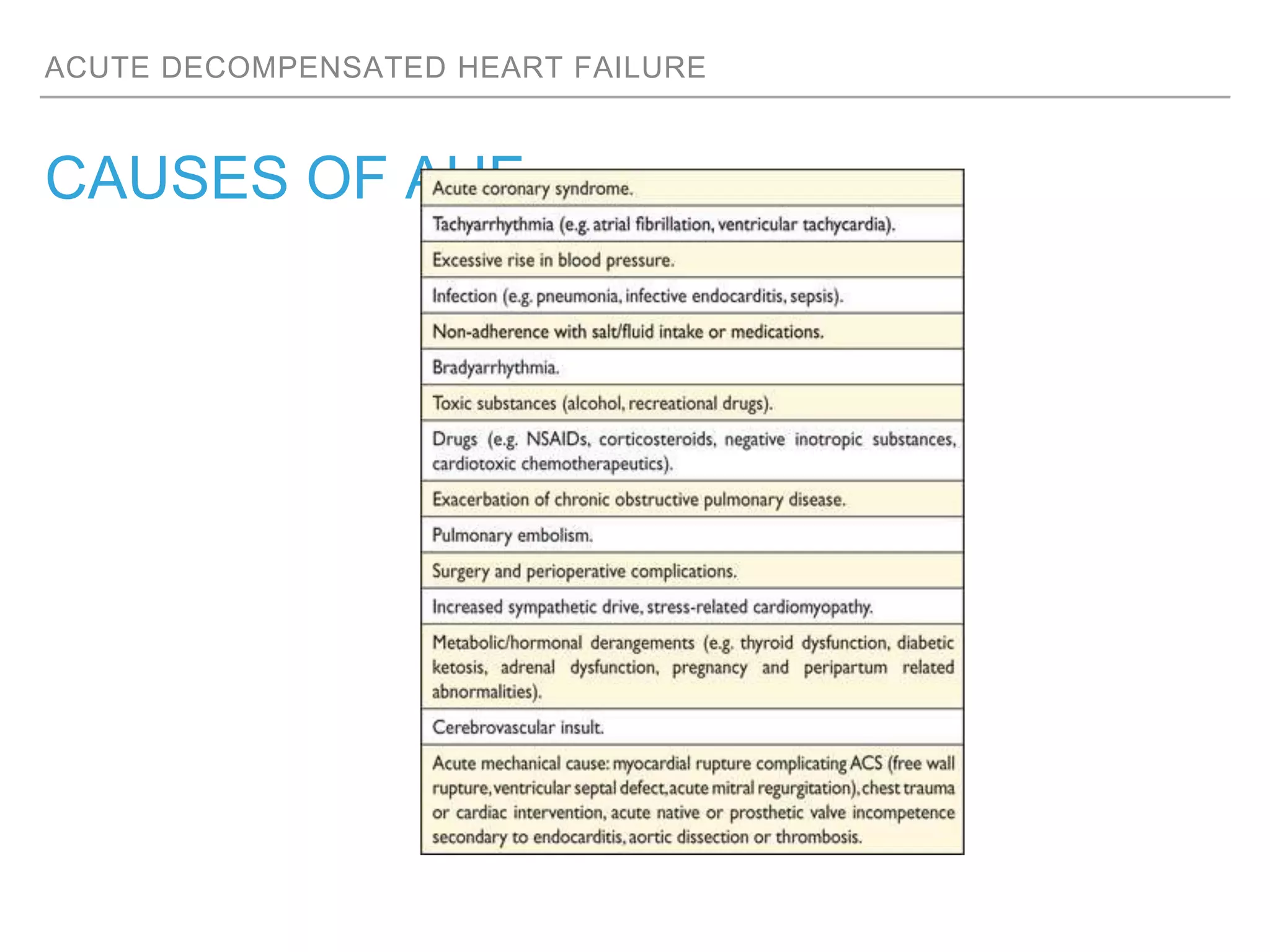





















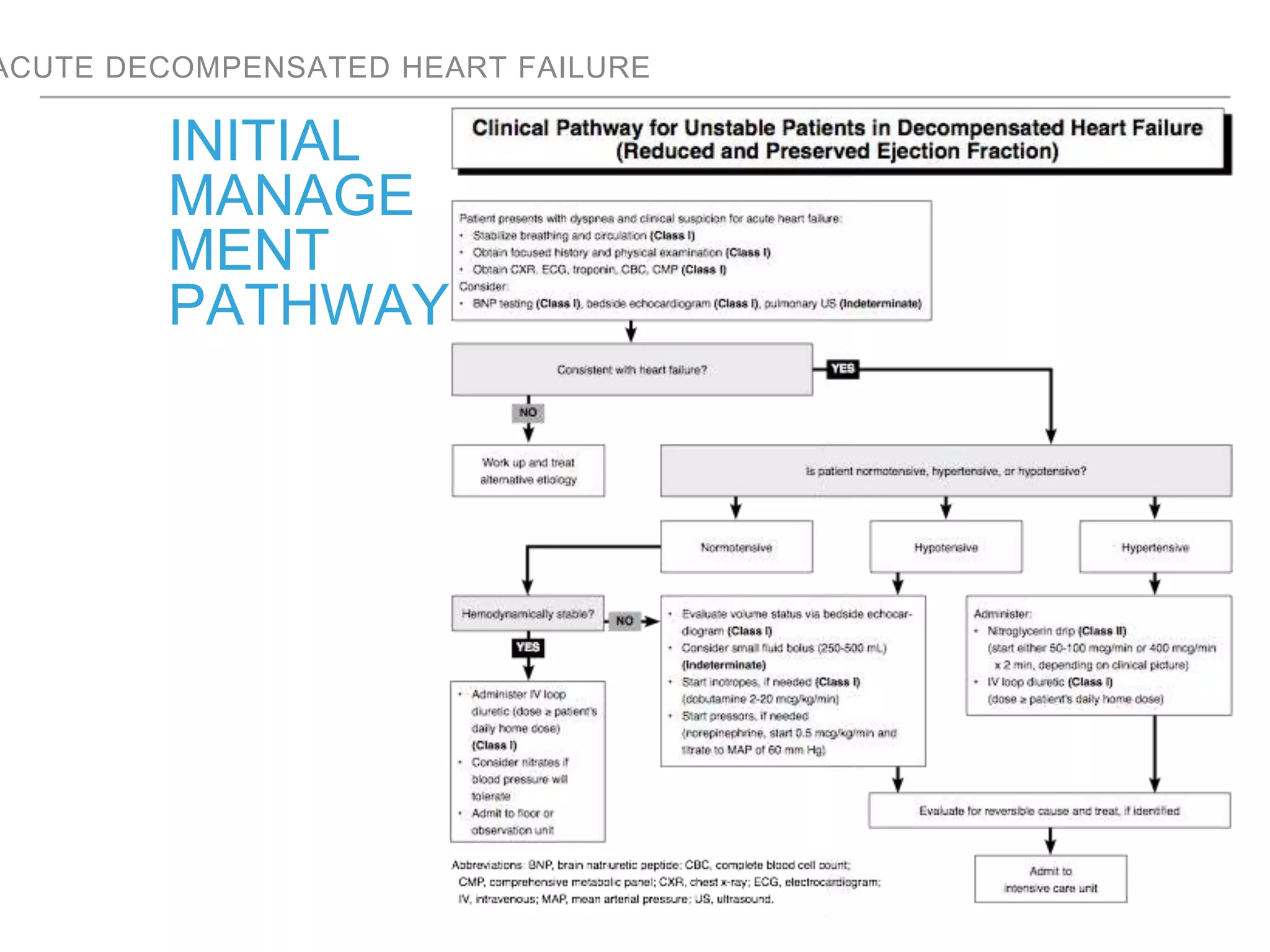































An overweight middle-aged man presented with acute shortness of breath, elevated blood pressure, coarse lung sounds, low oxygen saturation, and leg swelling. His initial evaluation found signs of severe congestive heart failure including pulmonary edema. Further assessment is needed to determine the underlying cause, guide treatment, and classify the type and severity of heart failure.




























![[20170216][Journal Club][Enhanced recovery pathways versus standard care afte...](https://cdn.slidesharecdn.com/ss_thumbnails/20170216journalclub-171114232901-thumbnail.jpg?width=640&height=640&fit=bounds)














































































