
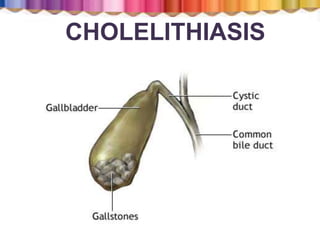
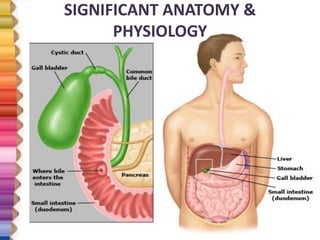
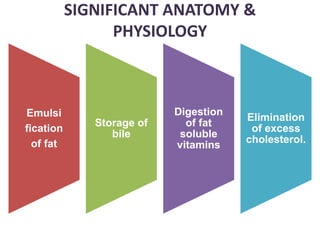
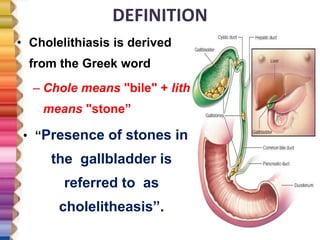
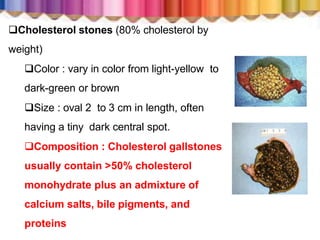
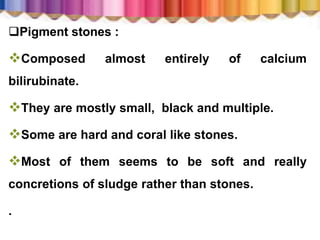
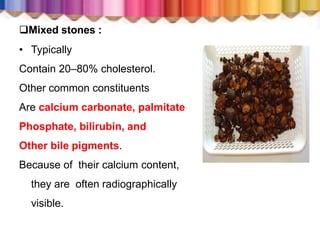



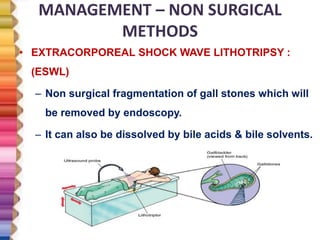
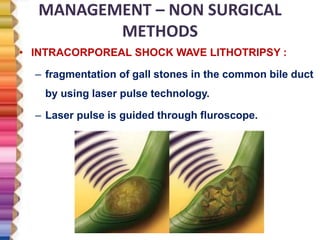
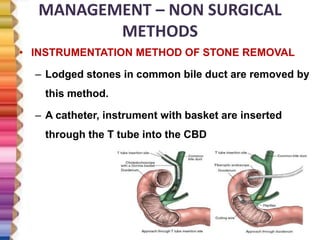
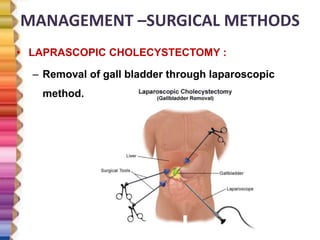
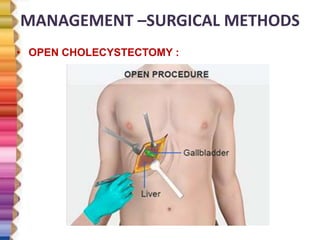
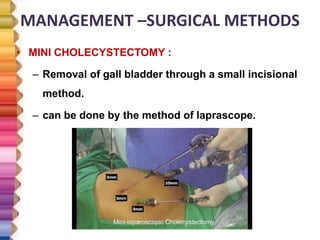
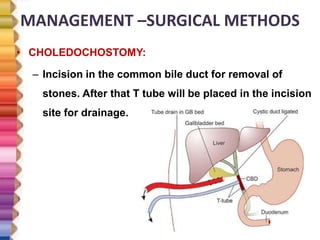
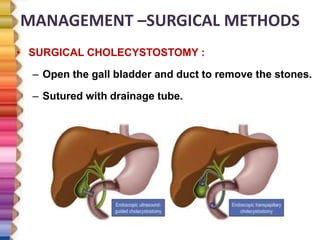
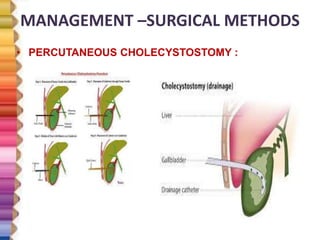


This document provides a case history and overview of cholelithiasis (gallstones). It begins with the case history of a 55-year-old male admitted with abdominal pain and vomiting who was diagnosed with acute gangrenous cholecystitis based on imaging. It then discusses the anatomy and physiology of the gallbladder, definitions and classifications of gallstones, risk factors, pathogenesis, clinical manifestations, diagnostic evaluations, and management. Management options discussed include nutritional therapy, pharmacological therapy, non-surgical methods like lithotripsy, and surgical methods like laparoscopic cholecystectomy.










































































