Dr Mohamed Shatat,MD
Professor of Internal Medicine
Minia University
Gall bladder Disorders
2.
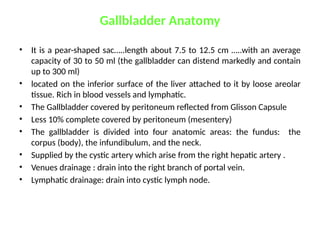
Gallbladder Anatomy
• Itis a pear-shaped sac…..length about 7.5 to 12.5 cm …..with an average
capacity of 30 to 50 ml (the gallbladder can distend markedly and contain
up to 300 ml)
• located on the inferior surface of the liver attached to it by loose areolar
tissue. Rich in blood vessels and lymphatic.
• The Gallbladder covered by peritoneum reflected from Glisson Capsule
• Less 10% complete covered by peritoneum (mesentery)
• The gallbladder is divided into four anatomic areas: the fundus: the
corpus (body), the infundibulum, and the neck.
• Supplied by the cystic artery which arise from the right hepatic artery .
• Venues drainage : drain into the right branch of portal vein.
• Lymphatic drainage: drain into cystic lymph node.
3.
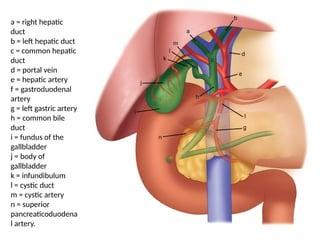
a = righthepatic
duct
b = left hepatic duct
c = common hepatic
duct
d = portal vein
e = hepatic artery
f = gastroduodenal
artery
g = left gastric artery
h = common bile
duct
i = fundus of the
gallbladder
j = body of
gallbladder
k = infundibulum
l = cystic duct
m = cystic artery
n = superior
pancreaticoduodena
l artery.
4.
Gallbladder Physiology
• Bileis mainly composed of water (97%), bile salts
(1-2%), (1%) phospho-lipids, cholesterol, bile
pigments, and electrolytes.
• Bile is alkaline and PH 5.7 – 8.6.
• The rate of bile secretion is 40 cc / hour.
• The normal adult consuming an average diet
produces within the liver 500 to 1000 ml of bile a
day.
5.
Gallbladder Function
• Bilestorage.
• Bile concentration 5-10 times by active absorption
of water and sodium decreasing the bile volume
80-90%.
• Secretion of mucin = 20 ml /day.
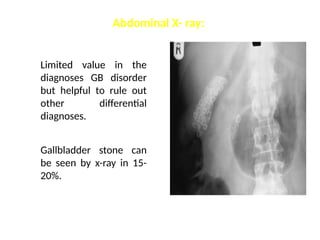
Limited value inthe
diagnoses GB disorder
but helpful to rule out
other differential
diagnoses.
Gallbladder stone can
be seen by x-ray in 15-
20%.
Abdominal X- ray:
9.
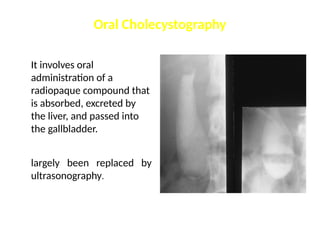
Oral Cholecystography
It involvesoral
administration of a
radiopaque compound that
is absorbed, excreted by
the liver, and passed into
the gallbladder.
largely been replaced by
ultrasonography.
10.
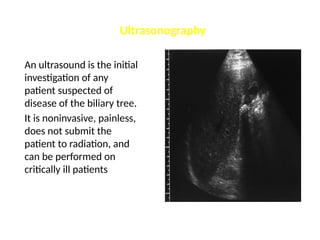
Ultrasonography
An ultrasound isthe initial
investigation of any
patient suspected of
disease of the biliary tree.
It is noninvasive, painless,
does not submit the
patient to radiation, and
can be performed on
critically ill patients
11.
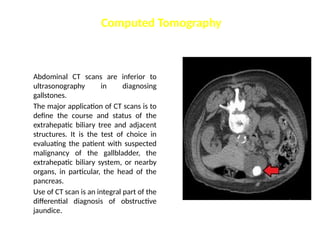
Abdominal CT scansare inferior to
ultrasonography in diagnosing
gallstones.
The major application of CT scans is to
define the course and status of the
extrahepatic biliary tree and adjacent
structures. It is the test of choice in
evaluating the patient with suspected
malignancy of the gallbladder, the
extrahepatic biliary system, or nearby
organs, in particular, the head of the
pancreas.
Use of CT scan is an integral part of the
differential diagnosis of obstructive
jaundice.
Computed Tomography
12.
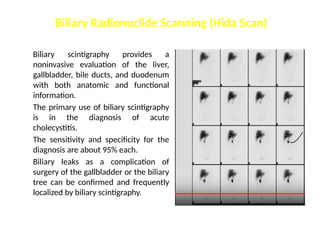
Biliary scintigraphy providesa
noninvasive evaluation of the liver,
gallbladder, bile ducts, and duodenum
with both anatomic and functional
information.
The primary use of biliary scintigraphy
is in the diagnosis of acute
cholecystitis.
The sensitivity and specificity for the
diagnosis are about 95% each.
Biliary leaks as a complication of
surgery of the gallbladder or the biliary
tree can be confirmed and frequently
localized by biliary scintigraphy.
Biliary Radionuclide Scanning (Hida Scan)
13.
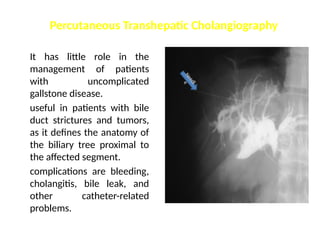
It has littlerole in the
management of patients
with uncomplicated
gallstone disease.
useful in patients with bile
duct strictures and tumors,
as it defines the anatomy of
the biliary tree proximal to
the affected segment.
complications are bleeding,
cholangitis, bile leak, and
other catheter-related
problems.
Percutaneous Transhepatic Cholangiography
N
e
e
d
l
e
14.
Magnetic Resonance Imaging
Ithas a sensitivity and specificity of 95 and 89%, respectively, at
detecting choledocholithiasis. MRI with magnetic resonance
cholangiopancreatography (MRCP) offers a single noninvasive
test for the diagnosis of biliary tract and pancreatic disease
15.
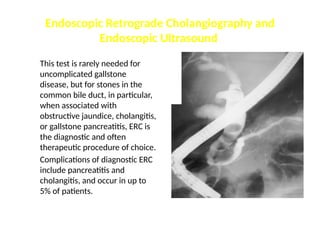
Endoscopic Retrograde Cholangiographyand
Endoscopic Ultrasound
This test is rarely needed for
uncomplicated gallstone
disease, but for stones in the
common bile duct, in particular,
when associated with
obstructive jaundice, cholangitis,
or gallstone pancreatitis, ERC is
the diagnostic and often
therapeutic procedure of choice.
Complications of diagnostic ERC
include pancreatitis and
cholangitis, and occur in up to
5% of patients.
20.
Gallstone Disease
Prevalence andIncidence :
• Gallstone disease is one of the most common problems
affecting the digestive tract (Autopsy reports have
shown a prevalence of gallstones from 11 to 36%.).
• The prevalence of gallstones is related to many factors:
• age, gender, and ethnic background
• Obesity, pregnancy, dietary factors,
• Crohn's disease, terminal ileal resection, gastric
surgery
• hereditary spherocytosis, sickle cell disease, and
thalassemia
21.
Types of gallstone
•Cholesterol stones ()
• Pigment stones ()
• Mixed ()
Epidemiology
• Fat, Fair, Female, Fertile, Fourty inaccurate, but reminder of the
typical patient
• F:M = 2:1
• 10% of British women in their 40s have gallstones
• Genetic predisposition – ask about family history
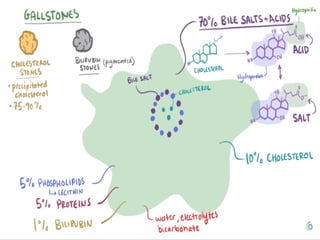
Gallstones
22.
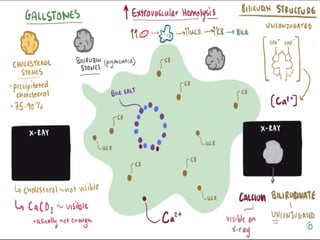
Composition of bile
•Bilirubin (by-product of haem degradation)
• Cholesterol (kept soluble by bile salts and lecithin)
• Bile salts/acids (cholic acid/chenodeoxycholic acid):
mostly reabsorbed in terminal ileum(entero-hepatic
circulation).
• Lecithin (increases solubility of cholesterol)
• Inorganic salts (sodium bicarbonate to keep bile
alkaline to neutralise gastric acid in duodenum)
• Water (makes up 97% of bile)
Pathogenesis
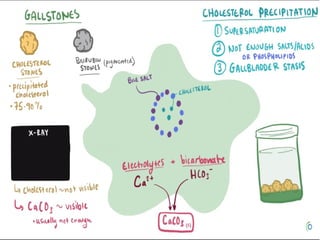
23.
Cholesterol
Imbalancebetween bile salts/lecithin and cholesterol allows
cholesterol to precipitate out of solution and form stones OR stasis
Pigment
Occur due to excess of circulating bile pigment (e.g. Heamolytic
anaemia)
Mixed
Same pathophysiology as cholesterol stones
Other Factors
Stasis (e.g. Pregnancy)
Ileal dysfunction (prevents re-absorption of bile salts)
Obesity and hypercholesterolaemia
Pathogenesis
24.
Cholesterol Stones
• Purecholesterol stones are uncommon and account for <10% of all stones.
They usually occur as single large stones with smooth surfaces.
• Most other cholesterol stones contain variable amounts of bile pigments
and calcium, but are always >70% cholesterol by weight. usually multiple,
of variable size. Colors range from whitish yellow and green to black.
• Most cholesterol stones are radiolucent; <10% are radiopaque.
• the primary event in the formation of cholesterol stones is supersaturation
of bile with cholesterol.
• Supersaturation almost always is caused by cholesterol hypersecretion
rather than by a reduced secretion of phospholipid or bile salts
25.
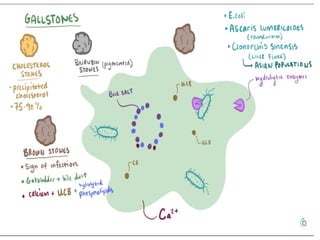
Pigment Stones
• Pigmentstones contain <20% cholesterol and are dark because of the
presence of calcium bilirubinate
• black and brown pigment stones have little in common and should be
considered as separate entities
• Black pigment stones are usually small, brittle, black, and sometimes
speculated, formed by supersaturation of calcium bilirubinate,
carbonate, and phosphate, most often secondary to hemolytic
disorders, and in those with cirrhosis. Like cholesterol stones, they
almost always form in the gallbladder.
• Brown stones : They may form either in the gallbladder or in the bile
ducts, usually secondary to bacterial infection (such as Escherichia
coli)caused by bile stasis. calcium bilirubinate and bacterial cell bodies
compose the major part of the stone.
Gallstone disease(and its related complications)
Gastritis/duodenitis
Peptic ulcer disease/perforated peptic ulcer
Acute pancreatitis
Right lower lobe pneumonia
MI
When there is RUQ pain…… all patients should get
Blood tests
AXR/E-CXR (to exclude perforation/pneumonia)
ECG
Differential Diagnosis of RUQ pain
39.
Can differentiate betweengallstone
complications based on:
• History
• Examination
• Blood tests
• FBC
• LFT
• CRP
• Clotting
• Amylase
Which Gallstone Complication?
40.
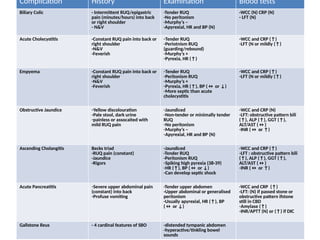
Complication History ExaminationBlood tests
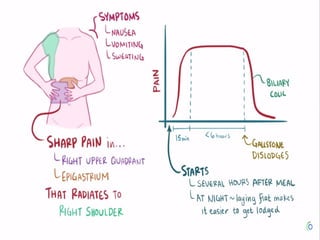
Biliary Colic - Intermittent RUQ/epigastric
pain (minutes/hours) into back
or right shoulder
- N&V
-Tender RUQ
-No peritonism
-Murphy’s –
-Apyrexial, HR and BP (N)
-WCC (N) CRP (N)
- LFT (N)
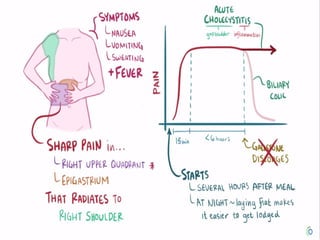
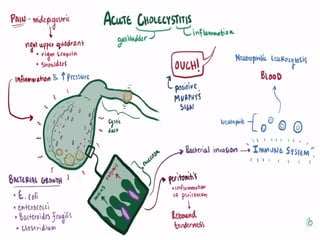
Acute Cholecystitis -Constant RUQ pain into back or
right shoulder
-N&V
-Feverish
-Tender RUQ
-Periotnism RUQ
(guarding/rebound)
-Murphy’s +
-Pyrexia, HR (↑)
-WCC and CRP (↑)
-LFT (N or mildly (↑)
Empyema -Constant RUQ pain into back or
right shoulder
-N&V
-Feverish
-Tender RUQ
-Peritonism RUQ
-Murphy’s +
-Pyrexia, HR (↑), BP (↔ or ↓)
-More septic than acute
cholecystitis
-WCC and CRP (↑)
-LFT (N or mildly (↑)
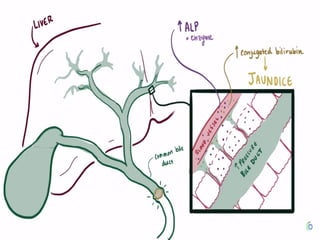
Obstructive Jaundice -Yellow discolouration
-Pale stool, dark urine
-painless or assocaited with
mild RUQ pain
-Jaundiced
-Non-tender or minimally tender
RUQ
-No peritonism
-Murphy’s –
-Apyrexial, HR and BP (N)
-WCC and CRP (N)
-LFT: obstructive pattern bili
(↑), ALP (↑), GGT (↑),
ALT/AST (↔)
-INR (↔ or ↑)
Ascending Cholangitis Becks triad
-RUQ pain (constant)
-Jaundice
-Rigors
-Jaundiced
-Tender RUQ
-Peritonism RUQ
-Spiking high pyrexia (38-39)
-HR (↑), BP (↔ or ↓)
-Can develop septic shock
-WCC and CRP (↑)
-LFT : obstructive pattern bili
(↑), ALP (↑), GGT (↑),
ALT/AST (↔)
-INR (↔ or ↑)
Acute Pancreatitis -Severe upper abdominal pain
(constant) into back
-Profuse vomiting
-Tender upper abdomen
-Upper abdominal or generalised
peritonism
-Usually apyrexial, HR (↑), BP
(↔ or ↓)
-WCC and CRP (↑)
-LFT: (N) if passed stone or
obstructive pattern ifstone
still in CBD
-Amylase (↑)
-INR/APTT (N) or (↑) if DIC
Gallstone Ileus - 4 cardinal features of SBO -distended tympanic abdomen
-hyperactive/tinkling bowel
sounds
41.
Pathogenesis
Stone intermittently obstructingcystic duct (causing pain)
and then dropping back into gallbladder (pain subsides)
USS confirms presence of gallstones
Treatment
Analgesia
Fluid resuscitation if vomiting
If pain and vomiting subside does not need admitting
Biliary Colic
42.
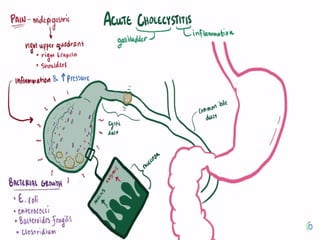
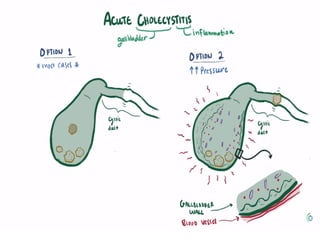
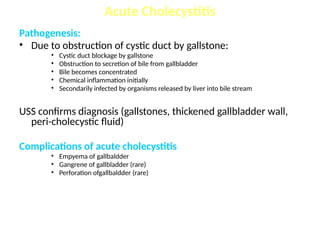
Pathogenesis:
• Due toobstruction of cystic duct by gallstone:
• Cystic duct blockage by gallstone
• Obstruction to secretion of bile from gallbladder
• Bile becomes concentrated
• Chemical inflammation initially
• Secondarily infected by organisms released by liver into bile stream
USS confirms diagnosis (gallstones, thickened gallbladder wall,
peri-cholecystic fluid)
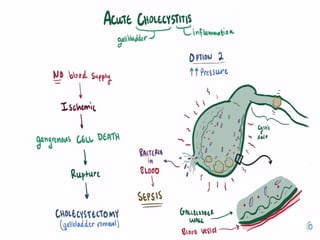
Complications of acute cholecystitis
• Empyema of gallbaldder
• Gangrene of gallbladder (rare)
• Perforation ofgallbaldder (rare)
Acute Cholecystitis
43.
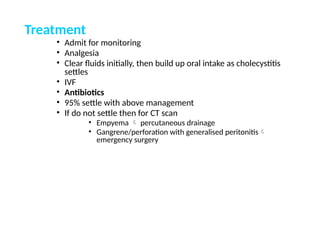
Treatment
• Admit formonitoring
• Analgesia
• Clear fluids initially, then build up oral intake as cholecystitis
settles
• IVF
• Antibiotics
• 95% settle with above management
• If do not settle then for CT scan
• Empyema percutaneous drainage
• Gangrene/perforation with generalised peritonitis
emergency surgery
44.
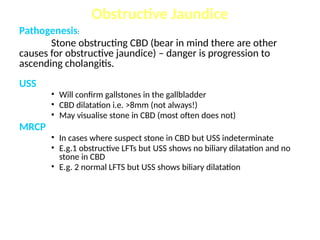
Pathogenesis:
Stone obstructing CBD(bear in mind there are other
causes for obstructive jaundice) – danger is progression to
ascending cholangitis.
USS
• Will confirm gallstones in the gallbladder
• CBD dilatation i.e. >8mm (not always!)
• May visualise stone in CBD (most often does not)
MRCP
• In cases where suspect stone in CBD but USS indeterminate
• E.g.1 obstructive LFTs but USS shows no biliary dilatation and no
stone in CBD
• E.g. 2 normal LFTS but USS shows biliary dilatation
Obstructive Jaundice
45.
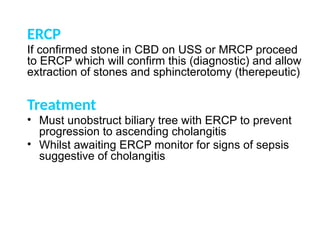
ERCP
If confirmed stonein CBD on USS or MRCP proceed
to ERCP which will confirm this (diagnostic) and allow
extraction of stones and sphincterotomy (therepeutic)
Treatment
• Must unobstruct biliary tree with ERCP to prevent
progression to ascending cholangitis
• Whilst awaiting ERCP monitor for signs of sepsis
suggestive of cholangitis
46.
Pathogenesis:
Stone obstructing CBDwith infection/pus proximal to
the blockage
Treatment
• ABC
• Fluid resuscitation (clear fuids and IVF, catheter)
• Antibiotics
• Pus must be drained* - this is done by decompressing
the biliary tree
• Urgent ERCP
• Urgent PTC – if ERCP unavailable or unsuccesful
Ascending Cholangitis
47.
Acute Pancreatitis
Pathogenesis
• Obstructionof pancreatic outflow
• Pancreatic enzymes activated within pancreas
• Pancreatic auto-digestion
USS: to confirm gallstones as cause of pancreatitis
• USS not good for visualising pancreas
CT: gold standard for assessing pancreas.
• Performed if failing to settle with conservative management to look for complications such as pancreatic necrosis
Treatment
• Analgesia
• Fluid resuscitation
• Pancreatic rest – clear fluids initially
• Identify underlying cause of pancreatitis
• 95% settle with above conservative management
• 5% who do no settle or deteriorate need CT scan to look for pancreatic necrosis
48.
Gallstone ileus
Pathogenesis:
• Gallstonecausing small bowel obstruction (usually obstructs in terminal ileum)
• Gallstone enters small bowel via cholecysto-duodenal fistula (not via CBD)
AXR – dilated small bowel loops
• May see stone if radio-opaque
Treatment
• NBM
• Fluid resuscitation + catheter
• NG tube
• Analgesia
• Surgery (will not settle with conservative management) – enterotomy + removal of stone
Diagnosis of gallstone ileus usually made at the time of surgery.
49.
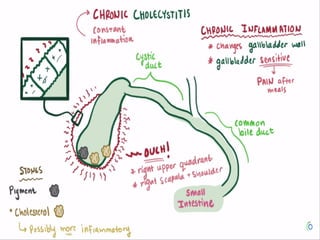
Chronic Cholecystitis
About twothirds of patients with gallstone disease present
with chronic cholecystitis
• characterized by recurrent attacks of pain( biliary colic). develops
when a stone obstructs the cystic duct
• vary from an apparently normal gallbladder with minor chronic
inflammation in the mucosa, to a shrunken, nonfunctioning
gallbladder with gross transmural fibrosis and adhesions to nearby
structures.
• The mucosa is initially normal or hypertrophied, but later becomes
atrophied, with the epithelium protruding into the muscle coat,
leading to the formation of the so-called Aschoff-Rokitansky sinuses
50.
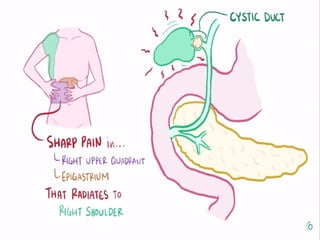
Clinical Presentation
Typical presentation:
•The chief symptom is pain (constant and increases in severity
over the first half hour or so and typically lasts 1 to 5 hours ).
located in the epigastrium or right upper quadrant and frequently
radiates to the right upper back or between the scapulae…The
pain is severe and comes on abruptly, typically during the night or
after a fatty meal…The pain is episodic. The patient suffers
discrete attacks of pain, between which they feel well.
• Physical examination may reveal mild right upper quadrant
tenderness during an episode of pain. If the patient is pain free,
the physical examination is usually unremarkable
• Laboratory values, such as WBC count and liver function tests, are
usually normal in patients with uncomplicated gallstones.
Atypical presentation ??
51.
• Asymptomatic gallstonesdo not require operation
• Indications
• A single complication of gallstones is an indication for
cholecystectomy (this includes biliary colic)
• After a single complication risk of recurrent
complications is high (and some of these can be life
threatening e.g. cholangitis, pancreatitis)
• Whilst awaiting laparoscopic cholecystectomy
• Low fat diet
• Dissolution therapy (ursodeoxycholic acid) generally
useless
Cholecystectomy
52.
Cholecystectomy
• All performedlaparoscopically
• Advantages:
• Less post-op pain
• Shorter hospital stay
• Quicker return to normal activities
• Disadvantages:
• Learning curve
• Inexperience at performing open cholecystectomies
53.
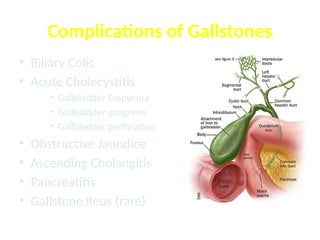
Tumors
• Carcinoma ofthe Gallbladder :
• Incidence :
• the fifth most common GI malignancy in Western
countries
• accounts for only 2 to 4% of all malignant GI tumors,
• two to three times more common in females than
males
• peak incidence is in the seventh decade of life
• It is an aggressive tumor (The overall reported 5-year
survival rate is about 5% ))
54.
Etiology
1. Gallstone isthe most important risk factor for
gallbladder carcinoma up to 95% of patients
with carcinoma of the gallbladder have
gallstones.
• Larger stones (>3 cm) are associated with a
10-fold increased risk of cancer.
2. Polypoid lesions (( particularly in polyps >10
mm)))
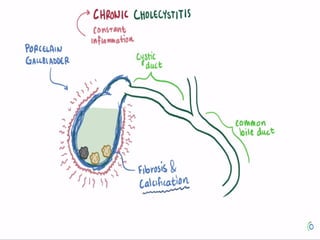
3. calcified "porcelain" gallbladder is associated
with >20% incidence of gallbladder carcinoma
4. choledochal cysts
5. exposure to carcinogens (azotoluene,
nitrosamines)
55.
Pathology
• 80 and90% of the gallbladder tumors are adenocarcinomas while
Squamous cell, adenosquamous, oat cell, and other anaplastic lesions
occur rarely
• spreads through the lymphatics, with venous drainage, and with direct
invasion into the liver
• Lymphatic flow from the gallbladder drains first to the cystic duct node
(Calot's), then the pericholedochal and hilar nodes, and finally the
peripancreatic, duodenal, periportal, celiac, and superior mesenteric
artery nodes.
• The gallbladder veins drain directly into the adjacent liver, usually
segments IV and V, where tumor invasion is common
• When diagnosed :
• about 25% of gallbladder cancers are localized to the gallbladder
wall
• 35% have regional nodal involvement and/or extension into
adjacent liver
• approximately 40% have distant metastasis
56.
• Clinical Manifestationsand Diagnosis
• Signs and symptoms of carcinoma of the gallbladder are generally
indistinguishable from those associated with cholecystitis and
cholelithiasis.
• More than one half of gallbladder cancers are not diagnosed before
surgery
• Laboratory findings are not diagnostic.
• Ultrasonography often reveals a thickened, irregular gallbladder wall
or a mass replacing the gallbladder. Ultrasonography may visualize
tumor invasion of the liver, lymphadenopathy, and a dilated biliary
tree . The sensitivity of ultrasonography in detecting gallbladder
cancer ranges from 70 to 100%
• A CT scan is an important tool for staging. identify a gallbladder mass
or local invasion into adjacent organs. demonstrate vascular invasion.
poor method for identifying nodal spread
• MRCP has evolved into a single noninvasive imaging method that
allows complete assessment of biliary, vascular, nodal, hepatic, and
adjacent organ involvement
• If diagnostic studies suggest that the tumor is unresectable, a CT scan
or ultrasound-guided biopsy of the tumor can be obtained to provide a
57.
TREATMENT
1. Surgery remainsthe only curative option for gallbladder cancer
2. no proven effective options for adjuvant radiation or chemotherapy for
patients with gallbladder cancer.
3. Tumors limited to the muscular layer of the gallbladder (T1) simple
cholecystectomy is an adequate treatment for T1 lesions and results in a near
100% overall 5-year survival rate
4. When the tumor invades the perimuscular connective tissue without
extension beyond the serosa or into the liver (T2 tumors)… extended
cholecystectomy should be performedincludes resection of liver segments IVB
and V, and lymphadenectomy
5. For tumors that grow beyond the serosa or invade the liver or other organs
(T3 and T4 tumors), there is a high likelihood of intraperitoneal and distant
spread. If no peritoneal or nodal involvement is found, complete tumor
excision with an extended right hepatectomy (segments IV, V, VI, VII, and VIII)
must be performed for adequate
6. An aggressive approach in patients who will tolerate surgery has resulted in
an increased survival for T3 and T4 lesions.
58.
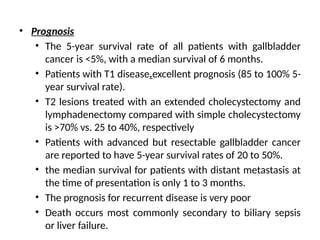
• Prognosis
• The5-year survival rate of all patients with gallbladder
cancer is <5%, with a median survival of 6 months.
• Patients with T1 disease.excellent prognosis (85 to 100% 5-
year survival rate).
• T2 lesions treated with an extended cholecystectomy and
lymphadenectomy compared with simple cholecystectomy
is >70% vs. 25 to 40%, respectively
• Patients with advanced but resectable gallbladder cancer
are reported to have 5-year survival rates of 20 to 50%.
• the median survival for patients with distant metastasis at
the time of presentation is only 1 to 3 months.
• The prognosis for recurrent disease is very poor
• Death occurs most commonly secondary to biliary sepsis
or liver failure.
59.
When should symptomaticgallbladder stones
be suspected?
The characteristic symptoms of gallbladder
stones, i.e. episodic attacks of severe pain in
the right upper abdominal quadrant or
epigastrium for at least 15-30 minutes with
radiation to the right back or shoulder and a
positive reaction to analgesics, should be
identified by medical history and physical
examination
60.
Should patients withasymptomatic gallstones
be treated?
Routine treatment is not recommended for
patients with asymptomatic gallbladder
stones
Is surgery indicated for gallbladder polyps?
Cholecystectomy should be performed in
patients with gallbladder polyps ≥1 cm without
or with gallstones regardless of their
61.
Is cholecystectomy indicatedin patients with
porcelain gallbladder?
Asymptomatic patients with porcelain
gallbladder may undergo cholecystectomy
Should prophylactic cholecystectomy be
offered to patients with hereditary
spherocytosis or sickle cell disease?
Cholecystectomy should be considered in
patients with hereditary spherocytosis and
sickle cell disease and concomitant
#3 Note: the situation of the hepatic bile duct confluence anterior to the right branch of the portal vein, the posterior course of the right hepatic artery behind the common hepatic duct.
#40 abdominal pain, vomiting, abdominal distention and absolute constipation