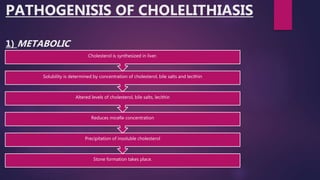
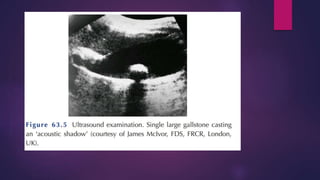
The document describes the anatomy and pathophysiology of gallstones (cholelithiasis). It details the anatomy of the gallbladder and biliary ductal system. It explains the formation of cholesterol stones and pigment stones, and lists risk factors for gallstone development. Potential complications are outlined, including biliary colic, cholecystitis, pancreatitis, and jaundice. Diagnosis involves ultrasound and liver function tests. Treatment typically involves cholecystectomy for symptomatic patients.