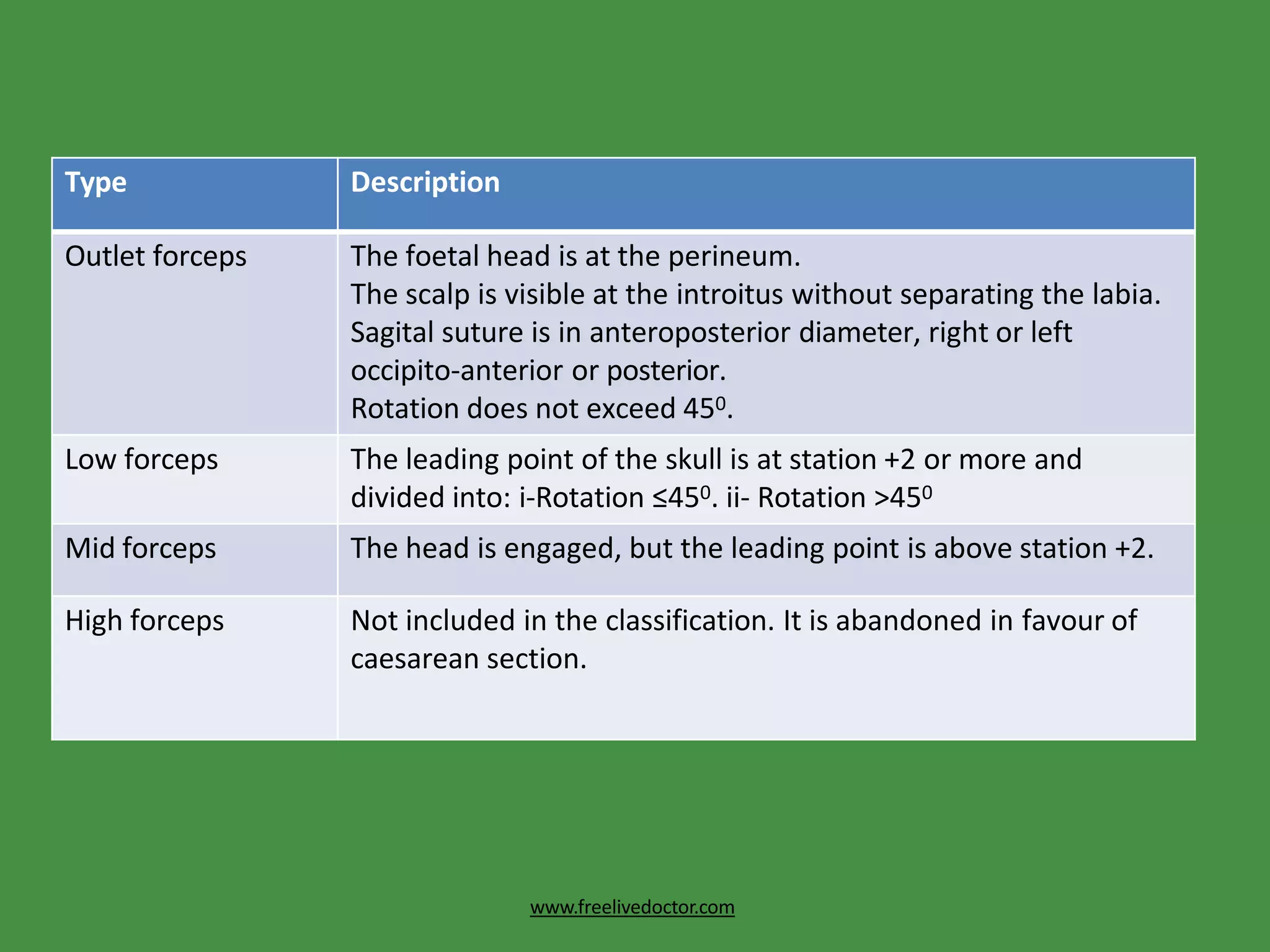
This document discusses forceps delivery, including definitions, types of forceps, indications for their use, techniques for application, and potential complications. Obstetric forceps are metal instruments used to extract the fetal head during delivery. They are indicated when delivery is prolonged or complicated by issues like fetal distress or maternal health conditions. Proper technique is important to minimize risks of injuries to the mother or baby. Complications can include lacerations, bone fractures, hemorrhage or problems for the infant like skull fractures or brain bleeding. Failed forceps require assessing the cause and may necessitate a C-section.