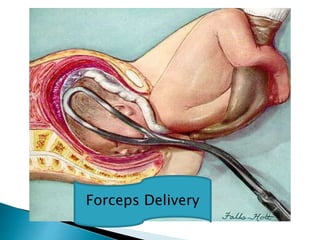
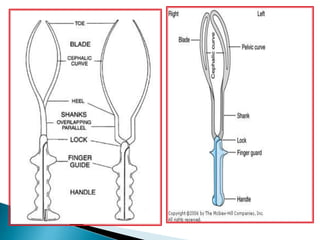
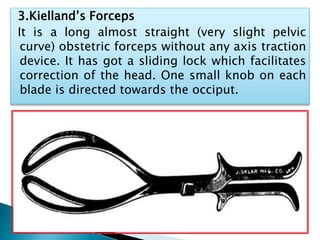
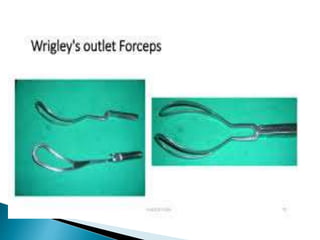
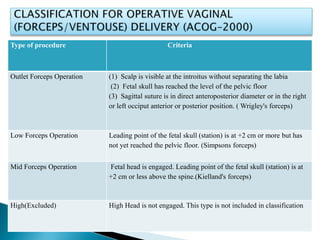
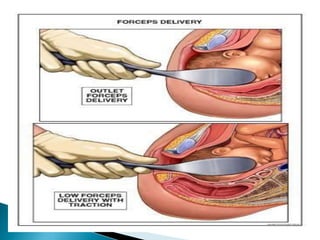
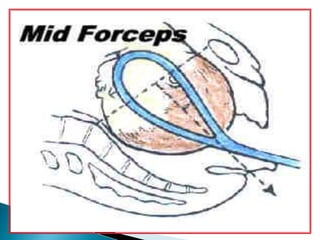
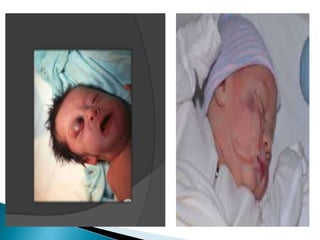
Operative vaginal delivery refers to any delivery assisted by vaginal operations such as forceps delivery, ventouse delivery, and destructive operations. Forceps delivery involves using obstetric forceps to extract the fetus when a vaginal birth is inadvisable or impossible without assistance. There are three main types of forceps used: long-curved forceps, short-curved forceps, and Kielland's forceps. Forceps delivery carries risks for both mother and infant if not performed correctly, including lacerations, hemorrhage, and injuries to the fetal head. Proper patient positioning, monitoring, and gentle controlled traction are important to minimize risks when forceps are clinically indicated for delivery assistance.