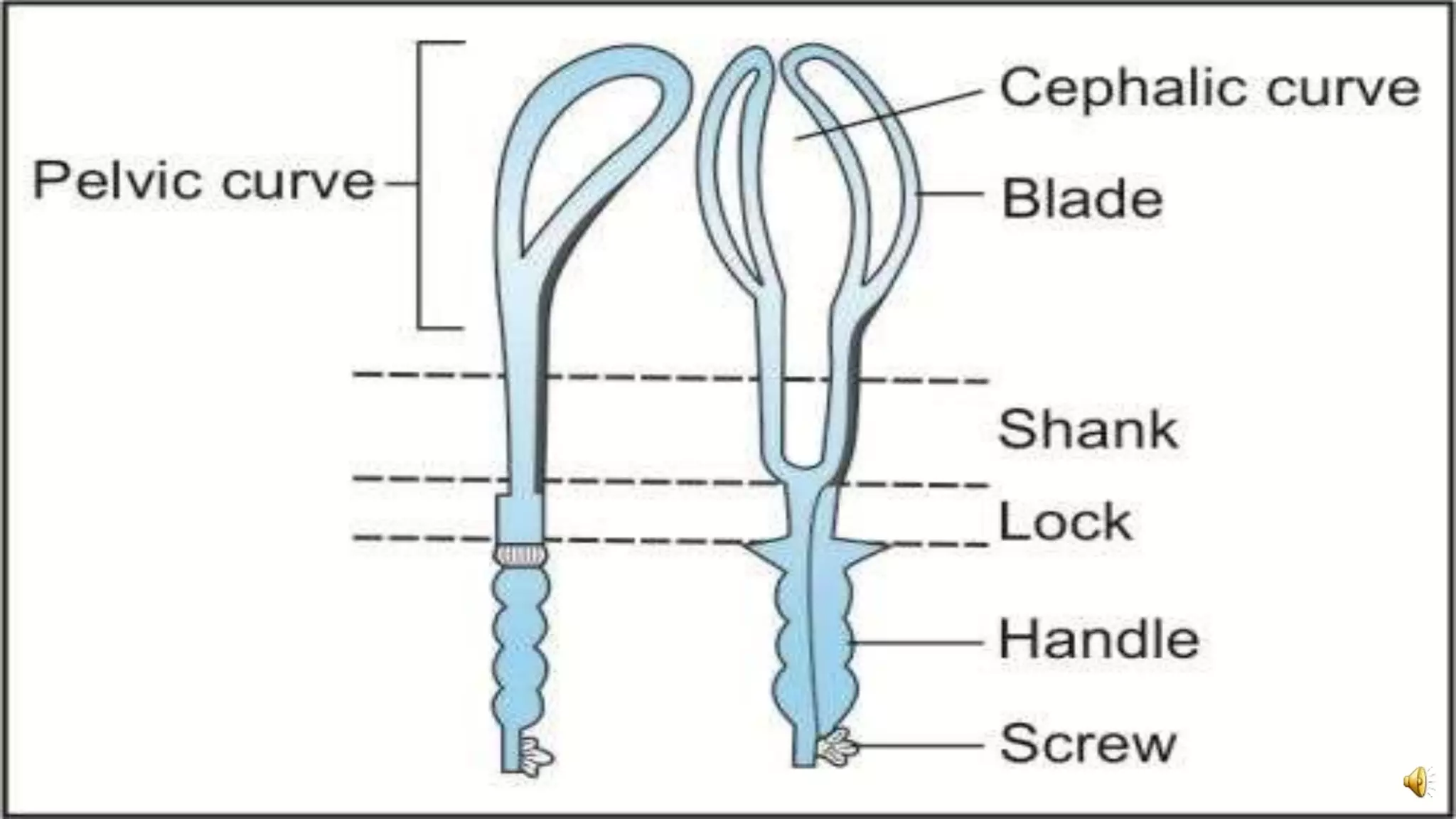
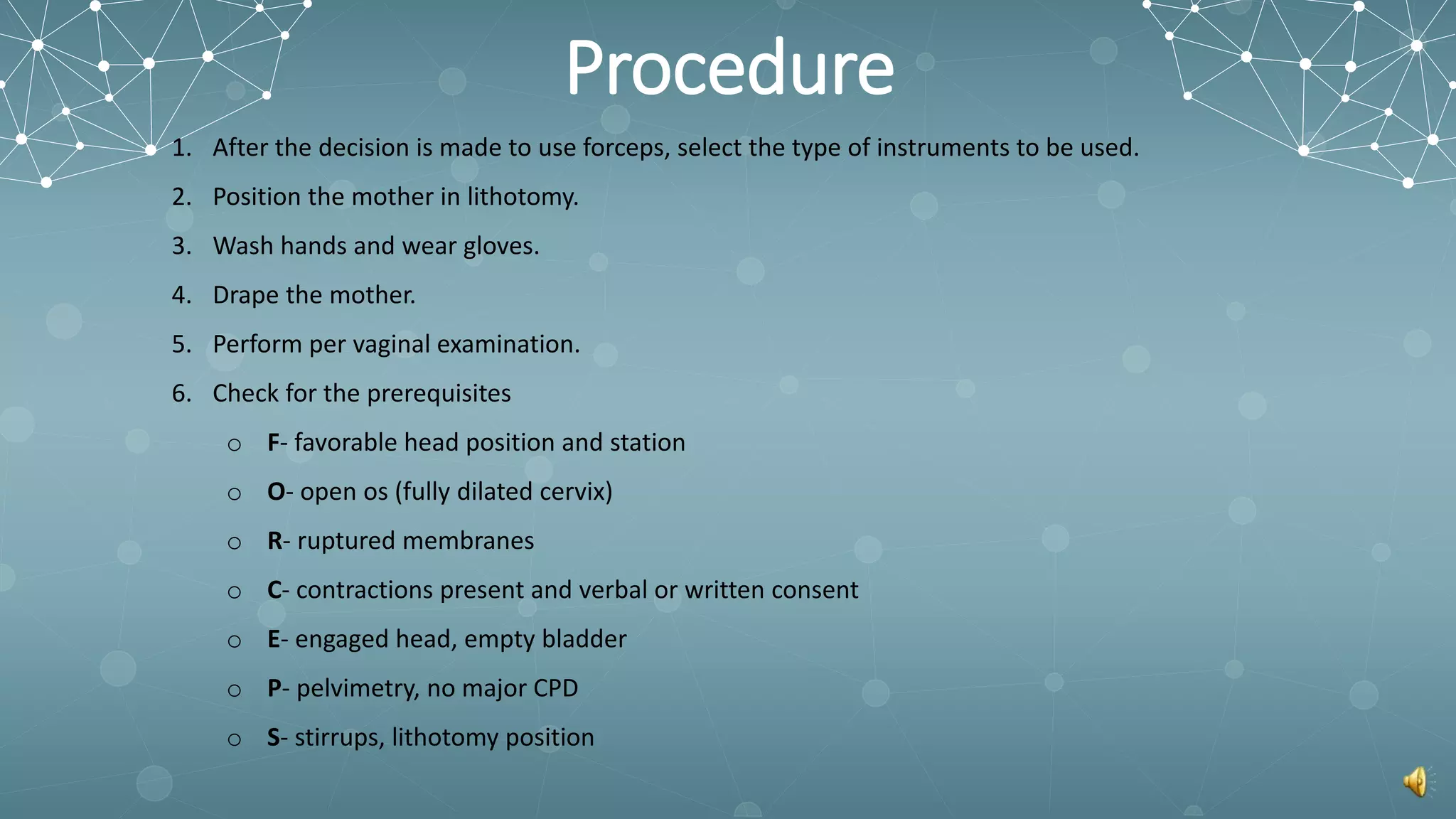
Forceps delivery is a procedure that uses obstetric forceps to assist in the extraction of a baby's head during childbirth. There are several requirements that must be met before a forceps delivery can be performed, including full cervical dilation and adequate anesthesia. The forceps procedure involves inserting the two curved blades of the forceps into the birth canal on either side of the baby's head. The blades are then locked together and gentle traction is applied to guide the head out. Potential complications include vaginal or cervical lacerations, postpartum hemorrhage, and injuries to the baby such as bruising or skull fractures.





















































![Operative_obstetrics_Presentation3[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/operativeobstetricspresentation31-251210093149-f8512b7d-thumbnail.jpg?width=640&height=640&fit=bounds)
































