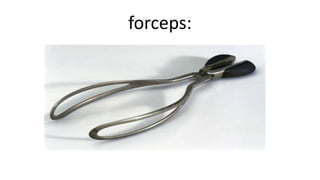
Forceps delivery and vacuum extraction are common operative vaginal delivery techniques used to expedite delivery when needed. Forceps have curved blades that grasp the fetal head, while vacuum extraction uses suction from a soft silicone cup placed on the fetal scalp. Both require the fetus to be fully engaged and have certain prerequisites checked before use, including maternal and fetal condition, cervical dilation, and anesthesia. Complications can include increased maternal and neonatal injury compared to spontaneous vaginal delivery, so these techniques aim to minimize risks while aiding delivery.





















































































![operative_vaginal_delivery[1].pptrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrr...](https://cdn.slidesharecdn.com/ss_thumbnails/operativevaginaldelivery1-241116225613-cf843d5e-thumbnail.jpg?width=640&height=640&fit=bounds)








































