The document describes obstetric forceps, including their construction, parts, classification, indications for use, prerequisites, and techniques for application. Specifically:
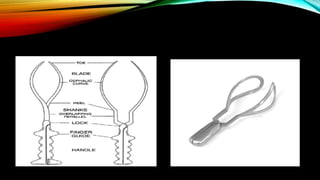
- Forceps consist of two curved branches with blades, a lock, and handles, designed to grasp and extract a fetus's head from the birth canal.
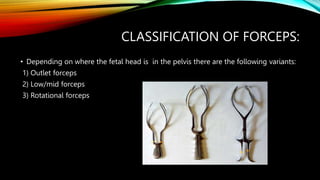
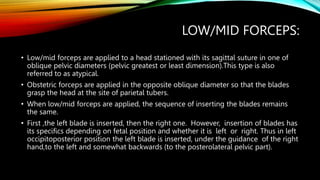
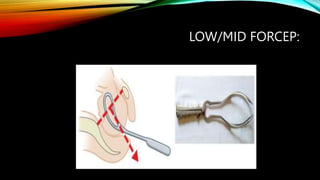
- They are classified by where the head is positioned, such as for outlet delivery when the head is at the pelvic floor or for low/mid delivery when the head is in the pelvis.
- Forceps delivery is indicated when maternal or fetal risks require rapid delivery, such as preeclampsia, fetal distress, or weak pushing. Certain prerequisites must be met for a safe forceps delivery.

























































![Operative_obstetrics_Presentation3[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/operativeobstetricspresentation31-251210093149-f8512b7d-thumbnail.jpg?width=640&height=640&fit=bounds)